Aid & Attendance: The Exam, the Evidence, and Why Claims Are Denied
Many A&A claims fail on documentation, not eligibility. The veteran qualifies, but the paperwork does not connect their limitations to the specific criteria the VA uses to decide. This guide explains what those criteria are, how the A&A exam differs from a standard C&P exam, and what the Board of Veterans' Appeals data shows about grants and denials.
What Is an A&A Medical Exam?
An Aid & Attendance medical exam is a specific type of VA examination focused on whether a veteran needs regular personal assistance or supervision to safely manage daily life. It is distinct from the standard Compensation & Pension (C&P) exam used to establish or rate a service-connected condition.
The primary document associated with A&A is VA Form 21-2680 (Examination for Housebound Status or Permanent Need for Regular Aid and Attendance). This form can be completed by a physician (VA or private) and documents the veteran's diagnoses, functional limitations, and need for assistance. The form is not the exam. The VA orders a separate A&A exam when it needs more information.
The Legal Standard: 38 CFR 3.352(a)
A&A eligibility is determined under 38 C.F.R. § 3.352(a), which lists the functional conditions that qualify a veteran for regular aid and attendance. The regulation does not require a veteran to meet all criteria. Any one is sufficient. The exact regulatory language states: "It is not required that all of the disabling conditions enumerated in this paragraph be found to exist before a favorable rating may be made."
The criteria under 38 C.F.R. § 3.352(a) are:
- 1 Dressing and grooming. Inability to dress or undress oneself, or to keep oneself ordinarily clean and presentable.
- 2 Prosthetic/orthopedic adjustment. Frequent need of adjustment of special prosthetic or orthopedic appliances which, because of the particular disability, cannot be done without aid. (Standard adjustable supports or back-laced items that anyone would need help with do not count.)
- 3 Feeding. Inability to feed oneself due to loss of coordination of the upper extremities or extreme weakness.
- 4 Toileting. Inability to attend to the wants of nature.
- 5 Supervision for hazards. Physical or mental incapacity that requires care or assistance on a regular basis to protect the veteran from hazards or dangers in their daily environment.
- + Permanently bedridden. The regulation also identifies permanent bedridden status as a separate basis for the determination. Being bedridden must be essential to the veteran's condition; a physician's recommendation to rest in bed for part of the day does not qualify.
Source: 38 C.F.R. § 3.352 (eCFR)
A&A vs. Standard C&P Exam
The two exam types serve different purposes and produce different outcomes. The difference matters. A&A decisions are not always made by medical professionals. They are often reviewed by Rating Veterans Service Representatives (RVSRs) who are not clinicians and who evaluate the documentation they receive.
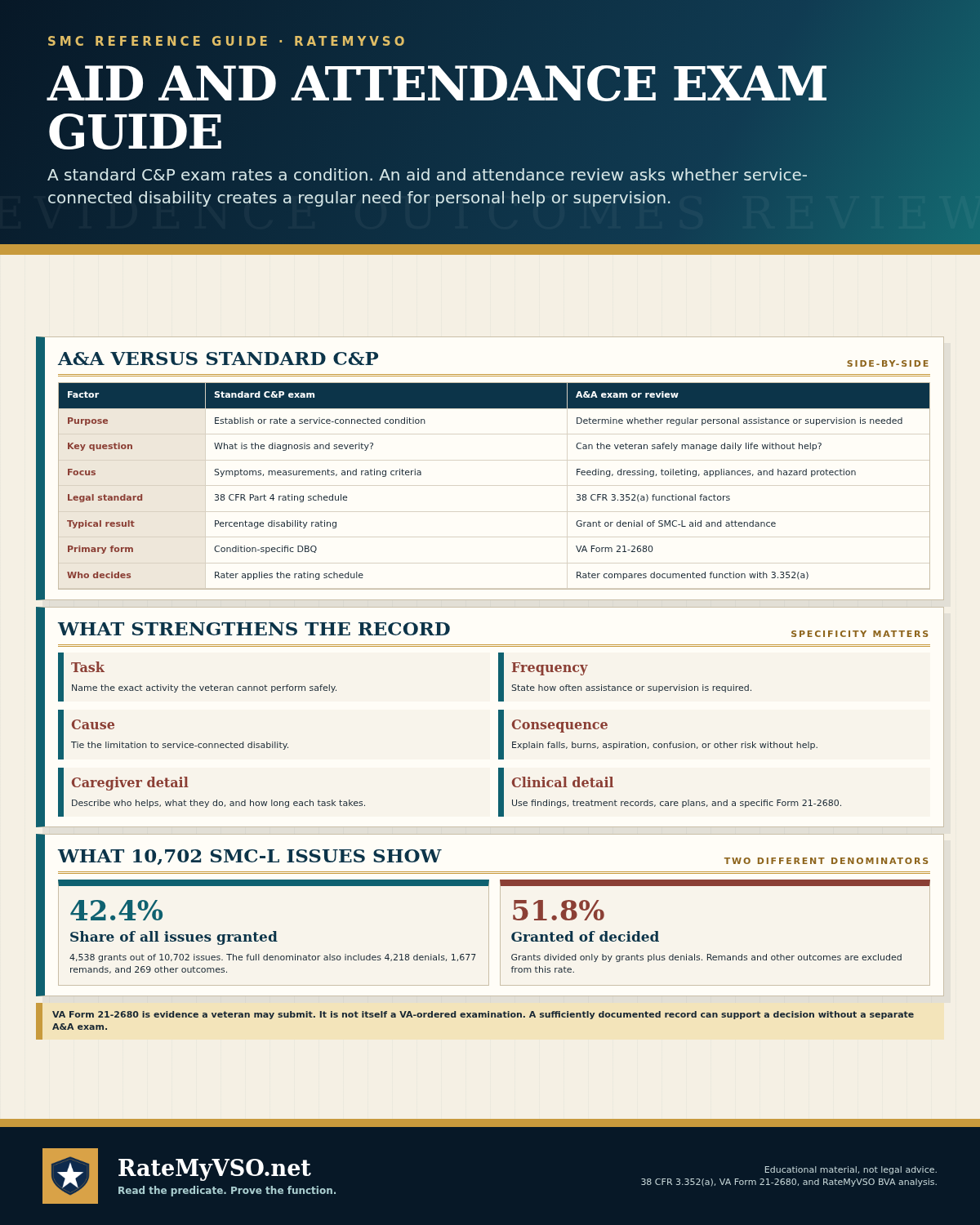
| Factor | Standard C&P Exam | A&A Exam |
|---|---|---|
| Purpose | Establish or rate a service-connected condition | Determine whether a veteran needs regular personal assistance or supervision |
| Key question | What is the diagnosis and severity? | Can the veteran safely manage daily life without help? |
| Focus | Symptoms, measurements, rating table criteria | Functional abilities: feeding, dressing, toileting, hazard awareness |
| Legal standard | VA Schedule for Rating Disabilities (38 CFR Part 4) | 38 C.F.R. § 3.352(a): activities of daily living |
| Outcome | Percentage disability rating | Grant or denial of SMC-L (A&A special monthly compensation) |
| Primary form | DBQ (Disability Benefits Questionnaire) | VA Form 21-2680 |
| Who reviews | Rating VSR applies rating tables | Rating VSR interprets functional limitations against § 3.352(a) |
When the VA Should Order an A&A Exam
A VA-ordered A&A exam is not required in every case. If the medical documentation (including a well-completed VA Form 21-2680) is sufficient to establish entitlement under 38 C.F.R. § 3.352(a), the VA can grant A&A without ordering a separate examination.
However, the VA's M21-1 adjudication manual describes when an A&A or housebound examination may be useful: when the evidence suggests a reasonable probability of entitlement but is not yet sufficient to grant the benefit. In that situation, the appropriate VA response is to order an exam, not to deny the claim without one.
VA Form 21-4138: Statement in Support of Claim
Some veterans and their representatives use VA Form 21-4138 (Statement in Support of Claim) to submit written statements alongside the 21-2680 that explicitly identify the functional criteria met under 38 C.F.R. § 3.352(a) and, where appropriate, note that if the rater finds the evidence insufficient to grant, an A&A examination should be ordered under the VA's duty to assist rather than a denial issued.
This approach creates a documented record of the veteran's position, which is useful if the claim goes to a Higher-Level Review, because a DRO reviewing the file can identify whether the correct procedural step (ordering an exam) was skipped before the denial was issued.
Sources: VA Form 21-2680 · VA Form 21-4138 · 38 U.S.C. § 5103A (Duty to Assist) · M21-1, Part IV, Subpart i, Chapter 2, Section E (Examinations in Special Situations)
Evidence That Has Supported Grants at the Board
Of 10,702 SMC-L (Aid & Attendance) issues decided by the Board of Veterans' Appeals and included in the RateMyVSO BVA dataset, the following evidence types appear most frequently in the record:
What Makes a 21-2680 More Useful
VA Form 21-2680 asks the examining physician to document diagnoses, functional limitations, and whether the veteran needs regular assistance. The form's usefulness depends on how specifically it is completed:
- Generic statements like "patient has difficulty with ADLs" are less specific than statements tying each limitation to a criterion in 38 C.F.R. § 3.352(a)
- Statements describing what happens when the veteran attempts a task unsupported (falls, aspiration risk, burns, confusion) address the "hazards or dangers incident to the daily environment" criterion directly
- Frequency matters: the regulation requires a need for "regular" aid and attendance, not constant aid
- The physician should indicate whether the limitations are due to the service-connected conditions, not just age or non-SC conditions
Caregiver and Lay Statements
Caregiver statements and lay testimony (from the veteran or family members) documenting what daily life actually looks like (what the veteran cannot do alone, what assistance is provided and how often) appear in a significant portion of BVA A&A appeals. These statements are not a substitute for the 21-2680, but they can provide the contextual detail that a clinical form sometimes lacks.
BVA Grant Rates for A&A (SMC-L) Appeals
The following figures are drawn from Board of Veterans' Appeals decisions in the RateMyVSO BVA dataset.
SMC-L (Aid & Attendance) at the Board of Veterans' Appeals
Based on 10,702 SMC-L issues decided by the Board (granted 4,538 · denied 4,218 · remanded 1,677 · dismissed/continued 248). Excluding remands and dismissals, the grant-vs-denial rate is 51.8% granted / 48.2% denied.
Common denial themes cited in Board decisions
Counts reflect denial themes tagged in BVA decisions; a single decision may include multiple themes. A larger pool of "case-specific" denials (~2,915) is excluded here because those reasons don't cluster into a common pattern. Source: RateMyVSO BVA dataset (Board decisions, all years).
The 51.4% direct grant rate (and 60.7% grant-vs-denial rate) reflects A&A appeals that made it to the Board after an initial regional-office denial. These are cases that were strong enough to pursue but not strong enough to be granted earlier. The most common Board-identified denial themes involve specific functional criteria (bedridden status, self-care, loss of use), which reinforces that documentation specificity at the criterion level is what determines outcomes.
If Your A&A Claim Was Denied
A denial of A&A (SMC-L) is a rating decision subject to the standard VA appeals process. The most important first step is reviewing the decision letter for the specific reason cited.
Check whether an exam was ordered
If the decision letter denies A&A based on a rater's reading of the 21-2680 alone (without a VA-ordered A&A examination being part of the record), and you explicitly requested an exam prior to the denial, that may constitute a duty-to-assist error. Duty-to-assist errors can be raised in a Higher-Level Review (HLR), where a senior rater reviews the file for procedural errors. See the Higher-Level Review guide for how to identify and raise duty-to-assist errors in the HLR process.
Consider a supplemental claim with new evidence
If the denial is based on insufficient documentation rather than a procedural error, a Supplemental Claim (VA Form 20-0995) with new and relevant evidence (a more detailed 21-2680, a private physician statement specifically addressing 38 C.F.R. § 3.352(a) criteria, or a caregiver statement) is often more productive than an HLR on the same record. If a VA-ordered A&A exam was conducted and you believe it was inadequate, see the guide on challenging an inadequate C&P exam for the legal standard and procedural options.
Sources and references:
- 38 C.F.R. § 3.352: Aid and Attendance criteria (eCFR)
- 38 U.S.C. § 1114: SMC statutory authority (Cornell LII)
- 38 U.S.C. § 5103A: Duty to Assist (Cornell LII)
- VA Form 21-2680: Examination for Housebound Status or Permanent Need for Regular Aid and Attendance
- VA Form 21-4138: Statement in Support of Claim
- M21-1, Part IV, Subpart i, Chapter 2, Section E (Examinations in Special Situations), VA KnowVA adjudication manual
- RateMyVSO BVA Dataset, SMC-L appeals (Board of Veterans' Appeals decisions, all available years)
This guide is for educational purposes only and is not legal advice. Eligibility rules, form numbers, and regulatory language can change. Always verify at va.gov or ecfr.gov before filing. For individualized help with an A&A claim, find an accredited VSO representative. All RateMyVSO tools are free. We never sell anything.