VA Depression Claims Guide
Depression is one of the most common mental-health conditions the VA rates, and it is claimed under two diagnostic codes: diagnostic code 9434 for major depressive disorder and DC 9435 for unspecified depressive disorder. Both are rated on the exact same scale, the General Rating Formula for Mental Disorders at 38 CFR 4.130, the same 0/10/30/50/70/100 ladder used for PTSD and anxiety. The rating turns on how much the condition impairs your work and social life, not on a diagnosis label. This guide walks the whole path: how service connection works at a high level, how depression gets connected to your service (directly, or secondary to another condition including chronic pain, tinnitus, sleep apnea, TBI, or PTSD), the single combined mental rating rule, what evidence you need, why these claims get denied, a checklist before you file, what the claims process looks like step by step, how to read your decision letter, and what to do whether you win or you're denied.
What the VA Counts as Depression (major depressive disorder)
For VA purposes, depression is a diagnosed mental-health condition under 38 CFR 4.130. The diagnosis must conform to the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), which is required by 38 CFR 4.125. A diagnosis from a qualified provider is the threshold, feeling low or stressed is not enough on its own. Depression is claimed under two closely related codes, both rated on the same formula.
DC 9434, Major depressive disorder
The DSM-5 diagnosis of major depressive disorder (often called MDD or clinical depression). This is the most specific and most commonly claimed depression code.
DC 9435, Unspecified depressive disorder
The DSM-5 successor to the older "depressive disorder not otherwise specified" label. Used when a provider documents a depressive disorder that does not fully meet the criteria for a more specific diagnosis. It is rated on the identical 4.130 scale as 9434.
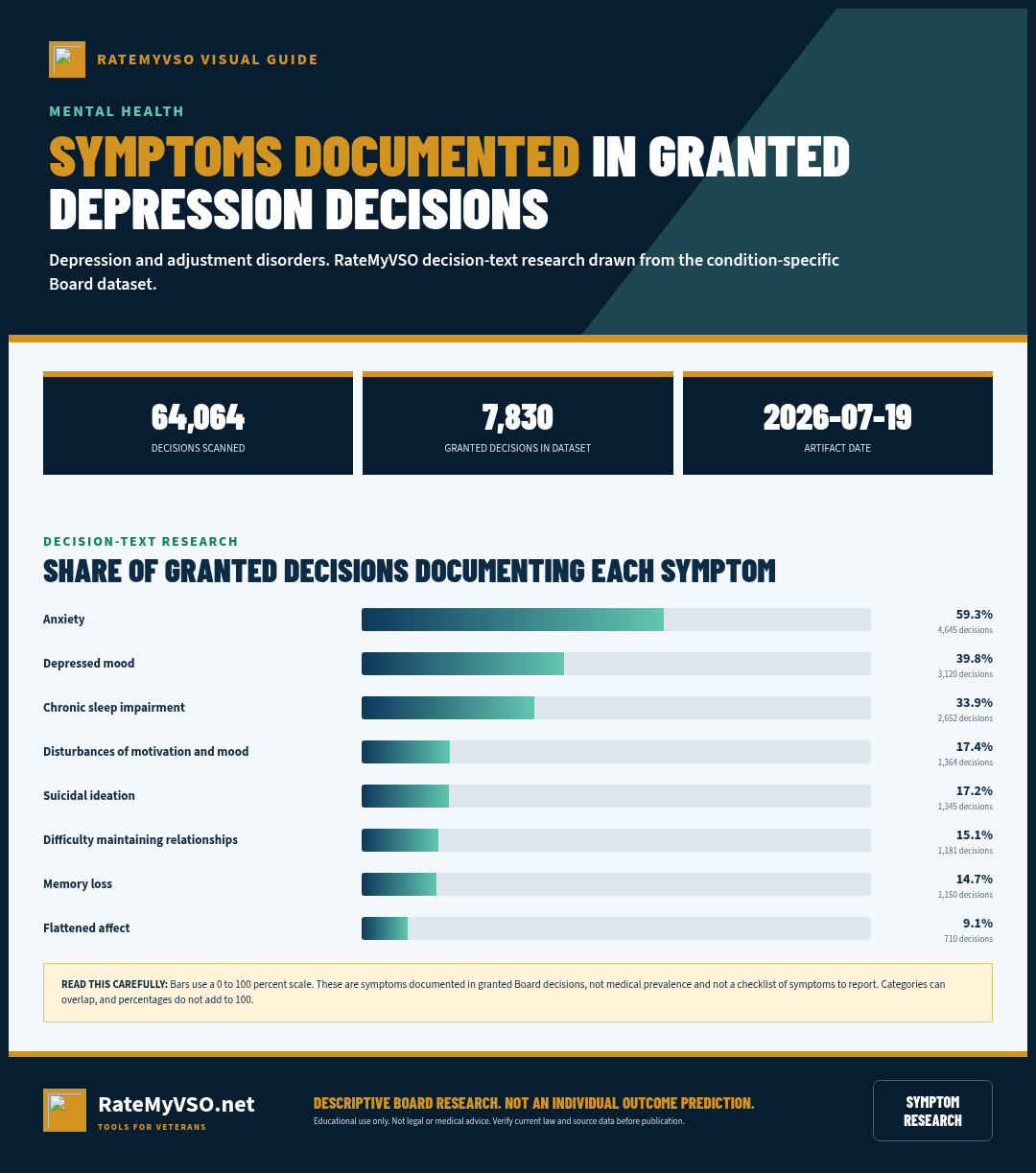
Symptoms Recorded in Granted Depression and adjustment disorders Decisions
We analyzed 7,830 granted Board decisions involving depression and adjustment disorders for symptoms named in sentences about the condition (rating-criteria recitations excluded). Descriptive of the published record, what the Board wrote down, not a checklist of what to report.
Detected by phrase-reading the decision text with condition-specific vocabularies. Source: Board of Veterans' Appeals decisions, RateMyVSO analysis.
ICD-10 Diagnosis Codes
The ICD-10 diagnosis codes most commonly used for DC 9434, Major depressive disorder (the kind on your medical records, decision letter, or C&P exam report). VA rates the disability and its residuals, not the diagnosis itself, so coding can vary.
How Service Connection Works, At a High Level
Before the specific pathways below, it helps to understand the three things every depression claim ultimately has to show. This is the same basic test the federal courts apply to any VA disability claim, just applied to this condition (38 CFR 3.303; Shedden v. Principi, 381 F.3d 1163 (Fed. Cir. 2004)).
- A current diagnosis. A mental-health professional's DSM-5 diagnosis of a depressive disorder, such as major depressive disorder or unspecified depressive disorder (38 CFR 4.125). Symptoms alone, without a formal diagnosis from a qualified provider, are not enough, and a veteran is not competent to diagnose their own depression.
- An in-service event, or a service-connected condition behind it. Something documented during service, such as a traumatic event, harassment, the stress of training or deployment, or a documented mental-health complaint, or a disability VA has already service-connected that caused or worsened your depression.
- A medical nexus. A qualified provider's opinion connecting your current depression to the in-service event or the service-connected condition, and explaining the reasoning, not just stating a conclusion.
How Depression (major depressive disorder) Gets Service Connected
Direct service connection
Direct service connection requires a current DSM-5 depression diagnosis, an in-service event or onset, and a medical nexus linking the two. We analyzed the Board's published decisions: depression is among the more frequently granted conditions on a direct basis, and a private nexus opinion in the file goes with a markedly higher grant rate, shown below. Consistent statements about when symptoms began, and any service record mentioning mental health, such as an in-service visit for a mental-health complaint or a separation exam noting depression or nightmares, corroborate a direct claim. The development manual for these claims is M21-1, Part V, Subpart iii, Chapter 13 (Mental Disorders).
No toxic-exposure presumptive
Depression has no presumptive pathway. There is no Agent Orange, no PACT Act or burn-pit, and no Camp Lejeune presumption that covers depression. It must be established on a direct or secondary basis. A depression diagnosis by itself, even with qualifying exposure history, does not trigger a presumption. The realistic routes are direct service connection and secondary service connection, described here.
Established pathways include:
Secondary to a Service-Connected Physical Condition
The strongest theory in the published data is depression caused or aggravated by an already service-connected condition, under 38 CFR 3.310. Chronic pain, tinnitus, sleep apnea, TBI, and migraines are common primaries. The Board's decisions show high grant rates for this direction: tinnitus to major depressive disorder was granted in approximately 77% of appeals (published BVA decisions, n = 83), and a service-connected lumbar or cervical strain to major depressive disorder was granted in approximately 79% of appeals (published BVA decisions, n = 50). A secondary claim requires a current depression diagnosis and a medical opinion stating that the service-connected condition caused or aggravated the depression. See secondary conditions and nexus letters.
Secondary to PTSD or Another Mental Condition
Depression is also commonly claimed secondary to PTSD. In published decisions, PTSD to major depressive disorder was granted in approximately 77% of appeals (published BVA decisions, n = 68). Note, however, the one-rating rule below: where PTSD and depression are both service connected, the VA assigns a single combined mental-health evaluation under 4.130 rather than separate percentages. The PTSD claims guide and the anxiety claims guide cover those conditions in depth.
One-Year Presumptive for a Psychosis (Rarely Controlling for Depression Alone)
Certain chronic diseases, including a psychosis, can be presumed related to service if they appear to a compensable degree within one year after separation (38 CFR 3.307, 38 CFR 3.309(a)). Board decisions have noted this rule exists, though most depression claims, including major depressive disorder and unspecified depressive disorder, are still decided on a direct or secondary basis rather than this presumption. Worth knowing about, but not a substitute for the direct or secondary pathways above.
Military Sexual Trauma (MST) and Other In-Service Trauma
Where the in-service event behind the depression is military sexual trauma or another form of personal trauma, a relaxed-evidence development pathway applies. The VA does not require proof that the event was reported at the time and may accept behavioral "markers" (such as transfer requests, performance drops, or new mental-health treatment) as evidence the event occurred, when a credible medical opinion supports the link. MST is not a presumption. It is a personal-trauma development pathway that can support depression as well as PTSD. The VA.gov page "Military sexual trauma and disability compensation" lists major depressive disorder among the conditions that can be service connected when caused by MST. The controlling development guidance is M21-1, Part VIII, Subpart iv, Chapter 1, Sections B and D.
What VA Looks For: Tests, Records, and Diagnostic Codes
Whether you are filing directly or secondary to another condition, the record VA actually reviews centers on a small set of documents and data points.
- The DSM-5 diagnosis itself: a mental-health evaluation identifying a specific depressive disorder, documented by a qualified provider and put in writing.
- Service treatment and personnel records: any note of a mental-health complaint, an emergency visit for "mental hygiene," a separation medical history mentioning depression or nightmares, or a documented in-service stressor. Ask VA to obtain your full service treatment and personnel records.
- Ongoing treatment and medication records: post-service VA and private mental-health records and medication history, which fill in the frequency, severity, and duration picture the rating formula requires, rather than a single day's presentation.
- The diagnostic codes involved: DC 9434 for major depressive disorder or DC 9435 for unspecified depressive disorder, plus whatever code applies to a condition you're connecting it to, for example DC 9411 (PTSD), DC 6847 (sleep apnea), or DC 8045 (TBI).
- The actual form the examiner fills out: a Disability Benefits Questionnaire (DBQ) specific to mental disorders, discussed in more detail later in this guide.
Evidence Cited in Published Depression and adjustment disorders Decisions
We analyzed 64,064 published Board decisions involving depression and adjustment disorders for condition-specific evidence, counting only case-specific mentions (boilerplate recitations excluded). "Favorable" is the share of decisions citing that evidence where every issue was granted or the outcome was mixed; the baseline across all these decisions is 66.2%, combining every diagnostic code below. Evidence appearing in a decision does not mean it decided the case. Descriptive of the published record, not a prediction.
By diagnostic code
These codes are grouped together above. They do not perform the same, so find your own code here rather than reading the combined figure. Codes retired in the schedule rewrites are left out, because their old decisions were judged under criteria that no longer apply.
Detected by phrase-reading the decision text with condition-specific vocabularies. Source: Board of Veterans' Appeals decisions, RateMyVSO analysis.

Board Grants, Dissected
The Board decisions below show major depressive disorder granted on a direct basis, meaning the Board found the condition itself began in service or is otherwise directly tied to service, not just secondary to another condition. These cases are not binding on other veterans' claims, and the Board's reasoning in one case does not control the outcome in another. Still, the pattern in these grants shows what kind of evidence the Board found persuasive.
100 days of rehab, then depression that never lifted Citation A26038463 (April 24, 2026), hearing docket
The record: Service treatment records from July 2008 documented a psychiatric evaluation after the veteran spent over 100 days in medical rehabilitation. He was diagnosed in service with adjustment disorder with depressed mood, including suicidal ideation and sleep problems. After service, VA providers gave him varying diagnoses (anxiety disorder, other trauma disorder). A June 2021 VA examiner diagnosed other specified trauma and stressor-related disorder and, despite checking a box saying it was not service-connected, wrote a rationale stating it was at least as likely as not incurred in service. A September 2024 private psychologist diagnosed major depressive disorder with anxious distress and explained why a mood-disorder diagnosis fit better than a trauma-disorder diagnosis, citing the documented depressive episode in service.
Why it won: The Board found the VA examiner's checkbox answer inconsistent with the examiner's own written rationale, and gave the written rationale, which supported service incurrence, more weight than the checkbox. The Board then found the private psychologist's opinion most persuasive on the specific diagnosis because it clearly explained the process of differentiating a mood disorder from a trauma disorder. The Board denied PTSD in the same decision because no provider found the full PTSD criteria met.
Discharge over suspected homosexuality tied to decades of depression Citation A26037985 (April 23, 2026), evidentiary window not specified (hearing withdrawn)
The record: The veteran served from 1948 to 1951 and was investigated for "homosexuality," receiving an "undesirable" discharge. Service treatment records did not document psychiatric treatment. A November 2025 VA exam diagnosed major neurocognitive disorder but did not address the psychiatric claim. In January 2026, a private psychologist, D.W., completed a mental disorders exam, diagnosed major depressive disorder, and opined it was at least as likely as not related to the undesirable discharge, explaining that the veteran avoided treatment for decades believing he was not eligible for it because of his discharge status.
Why it won: The Board found the private opinion the most probative evidence linking the diagnosis to service, and resolved reasonable doubt in the veteran's favor. The Board noted the earlier VA exam had limited value because it addressed an unrelated claim and did not include a nexus opinion.
Combat deployment symptoms documented before discharge Citation A26037552 (April 22, 2026), Direct Review docket
The record: The veteran served in combat in Afghanistan. The VA had already conceded in-service treatment for anxiety and combat exposure. Service treatment records from May and June 2022, shortly before discharge, documented trouble sleeping, sleep paralysis, loss of motivation, and increased alcohol use after deployment. A March 2025 VA exam found no nexus but was inconsistent with other records and did not appear to review the full claims file. A physician assistant, T.C., completed a July 2024 telehealth DBQ finding that the veteran's anxiety, depression, and insomnia began in service and worsened over time.
Why it won: The Board gave the March 2025 VA exam no weight because it conflicted with other records and did not reflect a full file review. The Board found T.C.'s opinion, though brief, supported by the service treatment records and by post-service VA treatment records from shortly after discharge that documented the same symptoms. The Board also dismissed a separate PTSD claim because the AOJ had already granted it in a later rating decision.
Treating psychologist's opinions outweigh four negative exams Citation A26037505 (April 22, 2026), hearing docket
The record: The AOJ had already conceded an in-service stressor and favorably found diagnoses of PTSD and major depression. The veteran's treating psychologist wrote opinions in 2018, 2020, and 2025 stating the trauma she experienced in service was a major foundation of her chronic PTSD, anxiety, and depression, and that her major depressive disorder had been present since 1989, linked to military sexual trauma. Five VA compensation examinations between 2019 and 2021 reached negative conclusions.
Why it won: The Board found the treating psychologist's opinions adequate and probative because they gave clear conclusions with supporting data and reasoning tied to the conceded stressor. The Board found the five VA exams inadequate because none of them considered the conceded in-service stressor or addressed the treating psychologist's opinion. The Board gave the negative opinions minimal weight for that reason.
Live-round training incident, favorable findings on current diagnoses Citation A26037163 (April 21, 2026), Direct Review docket
The record: The AOJ had already made favorable findings that the veteran had multiple mental health diagnoses, including anxiety, insomnia, depression, and PTSD. The veteran described live rounds being fired at him during training and submitted a 2022 statement describing the trauma. A February 2025 VA exam found no nexus, reasoning that the veteran's separate EMT training made the cause of his mental health condition unclear.
Why it won: The Board found the February 2025 VA exam inadequate because it did not consider the veteran's statements or his own reported experience, only his EMT background, and gave it low weight. The Board found the veteran's statements about the training incident competent and credible and gave them high weight, along with lay statements showing continuity of symptoms since service. The Board found the evidence at least in equipoise and resolved doubt in the veteran's favor.
Why These Claims Get Denied
Beyond the general "no diagnosis" and "no nexus" reasons covered above, a few specific denial patterns show up often enough to call out on their own.
- No diagnosis ever reaches the file. Claims have failed entirely where no provider ever diagnosed a psychiatric condition, sometimes because a representative told the Board a private nexus opinion would be submitted and it never arrived. If you say evidence is coming, make sure it actually reaches VA within the deadline.
- A veteran's own belief about the diagnosis, without a doctor behind it. VA treats a mental-health diagnosis as a medical question a non-doctor cannot answer on their own. A veteran's personal sense that they have depression, without a formal DSM-5 diagnosis, does not carry the claim.
- Evidence that describes the wrong time period. When the actual dispute is over an earlier rating period or an earlier effective date, testimony or a private opinion describing only current symptoms is given little weight. What matters is evidence describing the specific period actually on appeal.
- Assuming constant symptoms alone raise the rating. The rating turns on how much your symptoms impair work and social functioning, not on how often you feel them. Ratings have been kept at a mid-tier level where the veteran held full-time work despite ongoing symptoms.
- Filing a second appeal on an issue that's already pending. This creates an impermissible concurrent election, and the Board must dismiss it. Track what you already have pending before you file again.
- An onset story that shifts. When a veteran's account of when symptoms began changes between statements, and the record repeatedly contradicts an in-service onset, that inconsistency itself becomes a reason for denial.
DC 9434 Rating Levels
Both DC 9434 (major depressive disorder) and DC 9435 (unspecified depressive disorder) are rated on the General Rating Formula for Mental Disorders below, verbatim from 38 CFR 4.130. Each tier describes a level of occupational and social impairment, followed by example symptoms. The examples are illustrations, not a checklist that must be matched item for item.
Go deeper: open the full DC 9434 breakdown- What the VA measures at your C&P mental exam
- Evidence that has won at the Board
- Inside the rater's playbook: grant, denial, and remand rates
- Secondary condition map
The same six tiers apply to DC 9435 (unspecified depressive disorder). Where a veteran has more than one service-connected mental-health condition, a single percentage from this ladder covers all of them combined, as explained in the one-rating section above.
Notes from the regulation:
- Note 2: Ratings under diagnostic codes 9201 to 9440, which include both 9434 and 9435, are evaluated using the General Rating Formula for Mental Disorders. Ratings under diagnostic codes 9520 and 9521 are evaluated using the General Rating Formula for Eating Disorders.
- DSM-5 basis: The nomenclature in this part of the rating schedule is based on the DSM-5, and the general rating formula for mental disorders in 4.130 is applied to it.
For a tier-by-tier walkthrough of how raters apply each level, the Mental Health Rating Formula page covers the 4.130 ladder in depth for every mental condition.
Pyramiding and Rating Separately
The VA's pyramiding rule at 38 CFR 4.14 prevents paying twice for the same symptoms. For mental health this rule has a specific consequence: a veteran does not receive a separate rating for each mental-health diagnosis. Depression, PTSD, anxiety, and any other condition rated under 38 CFR 4.130 are combined into one mental-health evaluation. Because all of these conditions are scored on the same occupational-and-social-impairment scale, separate percentages would be rating the same impairment more than once.
Under the Mittleider principle, when symptoms cannot be clearly separated between a service-connected mental disorder and another condition, those symptoms are attributed to the service-connected disorder, which works in the veteran's favor for the single combined rating. The general evaluation procedures, including assigning one evaluation for coexisting psychiatric diagnoses, are described in M21-1, Part V, Subpart ii, Chapter 3, Section D (Evaluating Disabilities). A genuinely separate condition with its own distinct, non-overlapping symptoms and its own diagnostic code (for example, migraine headaches rated under DC 8100) can still be rated separately, as long as the same symptoms are not counted twice.
Pitfalls and Common Mistakes
Patterns the Board's published decisions and the VA's manual surface most often.
Procedural pitfalls to watch for:
- No confirmed DSM-5 diagnosis: "no current diagnosis" is one of the most common denial reasons for both codes. 38 CFR 4.125 requires the diagnosis to conform to the DSM-5.
- No medical nexus opinion: the absence of a link to service or to a service-connected condition is the single largest denial driver.
- Expecting a separate rating per diagnosis: depression plus anxiety or depression plus PTSD yields one combined evaluation under 4.130 and 4.14, not two stacked percentages.
- Assuming a presumptive applies: no Agent Orange, PACT Act, or Camp Lejeune presumption covers depression. It must be established directly or as a secondary.
- Overlooking the secondary pathway: claiming depression only on a direct basis can miss that depression caused or aggravated by a service-connected condition such as chronic pain, tinnitus, or PTSD grants at roughly 77% or higher in published BVA decisions.
- Letting one exam define the rating: 4.130 calls for evaluation based on the frequency, severity, and duration of symptoms over time, so a single snapshot exam can understate true occupational and social impairment.
- For MST-based claims, assuming the event had to be formally reported: the VA accepts behavioral markers and lay evidence in lieu of an official report under the personal-trauma development rules.
Do's and Don'ts
A condensed version of everything above, in the order it actually matters when you sit down to build your file.
- Get evaluated and get a current DSM-5 diagnosis in writing before anything else.
- Get a nexus opinion that reviews your history and explains its reasoning, not a bare conclusion.
- Tell every provider and examiner, consistently, when your symptoms started.
- Ask VA to obtain your full service treatment and personnel records, and flag any mental-health note.
- Raise a secondary theory if you already have a service-connected condition that could plausibly have caused or worsened your depression.
- Document how depression affects your daily life and work, hygiene, self-care, isolation, missed work, suicidal thoughts, honestly and specifically.
- If you cannot work because of depression, ask your representative about TDIU and SMC.
- If you were denied before, file with new and relevant evidence rather than repeating what VA already considered.
- Don't assume a diagnosis or symptoms alone will win, you still need the in-service cause and the medical link.
- Don't rely on your own self-diagnosis, VA requires a formal DSM-5 diagnosis for a mental condition.
- Don't promise evidence you don't actually submit, follow up if a private opinion or record hasn't arrived yet.
- Don't let testimony about how you feel now stand in for evidence about an earlier period when that's what's actually on appeal.
- Don't expect a higher rating just because symptoms feel constant, the rating turns on how much they impair work and social functioning.
- Don't file a second appeal on an issue that's already pending, it will be dismissed as a duplicate.
- Don't expect a separate rating for each mental-health diagnosis, depression plus PTSD or anxiety gets one combined 4.130 rating.
How 38 CFR 4.130 and the One-Rating Rule Work
Depression does not have its own unique set of symptoms in the rating schedule. Instead, every mental-health condition rated under diagnostic codes 9201 through 9440, including both depression codes, is evaluated under one shared scale: the General Rating Formula for Mental Disorders at 38 CFR 4.130. Note 2 to 4.130 states this directly. That is the same formula that rates PTSD (DC 9411) and anxiety. The rating measures one thing: how much the condition impairs your occupational and social functioning, scored at 0, 10, 30, 50, 70, or 100 percent.
The single-rating rule for multiple mental diagnoses
Many veterans carry more than one mental-health diagnosis at once, for example depression plus PTSD, or depression plus anxiety. The VA does not stack these into separate percentages. Under 38 CFR 4.130 and the anti-pyramiding rule at 38 CFR 4.14, the VA assigns one combined evaluation covering all of a veteran's service-connected mental-health conditions together. The Board applies what is often called the Clemons and Mittleider principle: where symptoms overlap and cannot be cleanly attributed to one specific diagnosis, those symptoms are attributed to the service-connected disorder rather than split apart. The practical effect is that a veteran with depression and PTSD receives a single mental-health rating reflecting the total impairment, not a depression rating added to a PTSD rating.
A snapshot exam is not the whole picture
The regulation directs raters to evaluate the condition based on all the evidence of the frequency, severity, and duration of symptoms over time, not on a single day's presentation. A thin treatment record or one good day at a Compensation and Pension (C&P) exam can understate the true level of occupational and social impairment. Ongoing treatment notes and medication history fill in the longitudinal picture the formula calls for.
Evidence for a Depression Claim
We analyzed the Board's published decisions and found a private medical opinion is the highest-yield evidence for these claims. The grant-rate comparison for each code, with a private opinion in the file versus without, is shown in the panels under the service connection section above.
A DSM-5 diagnosis in writing: the threshold document. Get evaluated by a qualified mental-health provider and make sure the diagnosis, not just a description of symptoms, actually reaches your file.
Service treatment and personnel records: old service records are powerful. An in-service note of a mental-health complaint, an emergency visit, or a separation medical history mentioning depression or nightmares can corroborate a private opinion. Ask VA to obtain your full service treatment and personnel records.
Nexus opinion: a medical opinion from a treating provider or qualified clinician wins when it reviews your history and gives a clear, reasoned explanation, not a bare conclusion. A well-reasoned private questionnaire or report carries considerable weight when nothing in the record contradicts it. See our Nexus Letters Guide.
Consistent onset statements: telling your providers and examiner, consistently, when your symptoms started can carry a direct claim, especially when paired with a service record noting a mental-health complaint around the same time.
Documentation of daily-life impact: for the rating, details matter. Describe suicidal thoughts, isolation, missed work, and self-care or hygiene problems honestly and specifically, this is the evidence that supports a higher tier on the 4.130 ladder, not just service connection itself.
Quick Checklist Before You File
Bring these together before you submit anything.
- A current DSM-5 diagnosis of depression from a qualified provider, in writing.
- Your full service treatment and personnel records, with any mental-health note or separation-exam entry flagged.
- A nexus opinion that reviews your history and explains, in plain reasoning, how service caused or worsened your depression.
- If you already have a service-connected condition, ask a provider whether your depression is secondary to it.
- A written, consistent account of when your symptoms began, kept the same across every statement and exam.
- For a higher rating, documentation of suicidal thoughts, hygiene and self-care problems, isolation, and missed work.
- If you cannot work because of depression, ask your representative about TDIU and SMC.
- If you were denied before: new and relevant evidence for a Supplemental Claim, not just a repeat of what was already considered.
For the mechanics of actually submitting the claim, see the Standard Claim Guide and the Fully Developed Claim Guide (filing with all your evidence up front can speed up the decision).
The Claims Process, Step by Step
Once you file, your claim moves through a series of hand-offs. Understanding who does what helps you know who to contact, and what to expect, at each stage.
- You file the claim. Directly with VA, through VA.gov, or with the help of an accredited representative.
- VA acknowledges the claim and assigns it for development. A Veteran Service Representative (VSR) is assigned to gather your service treatment records, VA and private medical records, and any other evidence needed.
- The VSR orders a Compensation & Pension (C&P) exam if one is needed. Most depression claims require a mental-health exam, especially secondary claims where a nexus opinion is needed.
- The C&P exam is conducted. By a VA clinician or a contracted examiner, who completes a Disability Benefits Questionnaire (DBQ) documenting the diagnosis, severity, and, where relevant, a nexus opinion.
- The file goes to a Rating Veteran Service Representative (RVSR), the "rater." The rater reviews the complete file, including the exam results, and decides whether service connection is warranted and at what percentage.
- A senior reviewer may review the decision before it's finalized, depending on the complexity of the claim.
- VA issues the decision letter. This states whether the claim is granted or denied, the rating percentage if granted, and the reasons behind the decision.
- If you disagree, you choose an appeal lane. Higher-Level Review, Supplemental Claim, or a Board appeal, covered later in this guide.
Who's who: VSO vs. VSR vs. Rater vs. C&P Examiner
Your VSO
An accredited representative from a veterans service organization, or an accredited attorney or claims agent. Not a VA employee. Helps you prepare, gather evidence, and file, and can represent you through an appeal. Has no authority to decide your claim.
VSR (Veteran Service Representative)
VA staff who "develops" your claim: requests records, schedules the C&P exam, and assembles the file. Does not decide the rating.
Rater (RVSR)
VA staff who reviews the completed file and makes the actual decision, service connection or denial, and the percentage. This is the person whose judgment the decision letter reflects.
C&P Examiner
A VA clinician or a contracted medical examiner who conducts the exam and completes the DBQ. Documents findings and, where asked, a nexus opinion. Does not decide the claim.
For the full walkthrough of every stage with more detail, see Inside Your Claim and Claim Stages.
DBQs and Your C&P Exam
Depression is established and rated through clinical evaluation rather than a lab value. The records and forms the VA relies on include:
- The mental disorders C&P examination and DBQ. The standard form is DBQ 21-0960P-2, Mental Disorders (Other Than PTSD and Eating Disorders). The examiner assesses occupational and social impairment against the 38 CFR 4.130 General Rating Formula. See the DBQ guide.
- The PTSD DBQs, when the claim is trauma-based. The Initial PTSD DBQ (21-0960P-3) or Review PTSD DBQ (21-0960P-4) is used instead when the claimed disorder is trauma-based, including MST-related depression evaluated alongside or as PTSD.
- A DSM-5 diagnostic interview. 38 CFR 4.125 requires a diagnosis conforming to the DSM-5, with an assessment of symptom frequency, severity, and duration rather than a single snapshot.
- VA Form 21-0781, Statement in Support of Claim for Service Connection for PTSD or Mental Health Conditions Related to a Traumatic Event, which documents the in-service stressor, including a personal-assault or MST stressor.
- Treatment and medication records. Service treatment records plus post-service VA and private mental-health records and medication history. Antidepressant use bears directly on the 10% and 30% tiers of the formula.
- Lay and behavioral-marker evidence. Buddy and lay statements, and for MST stressors, behavioral markers where contemporaneous reporting may be absent.
Before your C&P exam, bring a clear, specific, and consistent account of your symptoms and when they started. Describe your worst days and how depression affects your daily function, hygiene, work, and relationships, not just how you feel on an average day. Be consistent with what's already in your medical records and prior statements. For a full walkthrough of what to expect and how to prepare, see the C&P Exam Prep Guide.
Reading Your Decision Letter, and What to Do If Denied
Your decision letter has two parts: a narrative section explaining the reasoning (often called "reasons and bases"), and a codesheet showing the actual rating percentage, the effective date, and the diagnostic code used. See the Reading Your Decision Letter Guide for how to find and interpret each part, or use the Letter Interpreter tool to upload your own letter and get a plain-English breakdown.
If your claim is denied, or the rating is lower than you expected, you have three main lanes:
- Supplemental Claim: refile with new and relevant evidence, such as a new nexus opinion or updated treatment records. See Supplemental Claim Guide.
- Higher-Level Review (HLR): a senior reviewer looks at the same evidence again for a difference of opinion, no new evidence is added. See HLR Guide.
- Board Appeal: your case goes to a Veterans Law Judge at the Board of Veterans' Appeals, with options for a direct review, an evidence docket, or a hearing. See Board Appeal Guide.
Not sure which lane fits your situation? See the Appeals decision guide for a side-by-side comparison of all three. To reopen a previously denied claim you must submit new and relevant evidence, simply resubmitting an old opinion or repeating an argument VA already considered is not enough, and the Board will refuse to reopen (38 CFR 3.2501).
After You Win: Rating, Effective Date, and Staying Connected
In many depression files, the veteran was already service connected, and the real dispute was the rating percentage or the effective date. A few patterns from the Board's published decisions are worth knowing.
- A 100% rating requires total occupational and social impairment. Suicidal ideation matters for the rating, but its weight depends on how serious and frequent it is. Daily ideation without a plan, alongside family support, has been found consistent with the 70% tier rather than the 100% tier.
- Constant symptoms alone don't guarantee a higher rating. The rating turns on how much your symptoms impair work and social life, not how often you feel them; ratings have been kept at a mid-tier level where a veteran held full-time work despite ongoing symptoms.
- Effective dates usually run from the date of your claim (or intent to file), or the date the increase is factually shown, whichever is later (38 CFR 3.400). An earlier date has been granted where the worsening was factually shown within the year before the claim, but denied where the record did not show the higher level until a later statement.
- Depression that alone prevents you from working can support TDIU and added SMC housebound pay, even without a 100% schedular rating. Ask your representative about this if depression keeps you from working.
- To reopen a previously denied claim, you need new and relevant evidence, not a resubmission of an opinion or argument VA already considered (38 CFR 3.2501).
Keep your treatment consistent. Continued follow-up with a mental-health provider and records showing ongoing treatment protects you if VA schedules a future reexamination. Not every rating gets reexamined; understand when a rating becomes protected from future review (including Permanent and Total status) and what to do if VA proposes to reduce it. See Protect Your Rating and Future Reexaminations for the specifics.
If your depression worsens after the initial grant, you can file for an increased rating. See the Rating Increase Guide.
Common Secondary Conditions
Depression sits at the center of two distinct secondary relationships. It can be the downstream condition (something else causes the depression), and it can be the upstream condition (the depression, or the medication used to treat it, causes something else). We analyzed the Board's published decisions for grant rates in both directions.
Conditions that cause depression (depression as the secondary)
These are claims where depression was argued as secondary to an already service-connected condition. We found each bar is the published BVA grant rate to DC 9434 (major depressive disorder), with the number of decisions below it:
Conditions depression causes (depression as the primary)
Depression itself drives downstream secondaries, often through symptom overlap or medication side effects. We found each bar is the published BVA grant rate for a condition claimed secondary to major depressive disorder:
For DC 9435 (unspecified depressive disorder), the pattern is similar: sleep apnea secondary to 9435 was granted in approximately 73% of appeals (n = 349), and migraine secondary to 9435 in approximately 80% of appeals (n = 42, small sample), per published BVA decisions. These figures describe what the Board's published decisions show across many veterans. They are not a prediction about any one claim. More on framing both directions is on the secondary conditions page.
Quick Reference Tables
Secondary Connection Pathways
| Primary Condition | Mechanism | Evidence Needed |
|---|---|---|
| PTSD (DC 9411) | Overlapping trauma-related mood symptoms; single combined mental rating applies once both are service connected | Nexus opinion + DSM-5 diagnosis of depression |
| Chronic pain / back or neck disability | Chronic pain's psychological toll contributing to depressive symptoms | Nexus opinion linking the pain condition to the depression |
| Tinnitus | Persistent ringing contributing to mood and sleep disruption | Nexus opinion + DSM-5 diagnosis |
| Sleep apnea (DC 6847) | Chronic sleep disruption contributing to depressive symptoms | Nexus opinion addressing the sleep-mood link |
| TBI (DC 8045) | Recognized neuropsychiatric sequela of brain injury | Nexus opinion + DSM-5 diagnosis |
| Military sexual trauma or other in-service trauma | Trauma-related onset; behavioral markers accepted in place of a formal report | Credible lay statement + supporting medical opinion |
From Filing to Decision: Who Does What
| Role | Does | Decides your rating? |
|---|---|---|
| VSO / accredited representative | Helps prepare, gather evidence, and file; represents you on appeal | No |
| VSR | Develops the claim: orders records and the C&P exam | No |
| C&P Examiner | Conducts the exam, completes the DBQ, may give a nexus opinion | No / but has a strong impact |
| Rater (RVSR) | Reviews the full file and decides service connection and percentage | Yes |
Frequently Asked Questions
Is depression rated differently from PTSD or anxiety?
I have both depression and PTSD. Do I get two separate ratings?
What is the difference between DC 9434 and DC 9435?
Is depression a presumptive condition under Agent Orange or the PACT Act?
Can depression be service connected as secondary to a physical condition?
My depression comes from military sexual trauma I never reported. Does that matter?
Can I get TDIU or SMC for depression without a 100 percent rating?
Related Tools and Guides
Sources
- 38 CFR 4.130, General Rating Formula for Mental Disorders (DC 9434 and DC 9435)
- 38 CFR 3.303, direct service connection, including 3.303(d) for a disease diagnosed after service
- 38 CFR 3.310, secondary service connection
- 38 CFR 3.307 and 38 CFR 3.309(a), one-year presumptive period for a psychosis
- 38 CFR 3.102 and 38 USC 5107(b), benefit of the doubt
- 38 CFR 4.125, DSM-5 diagnosis required for a mental disorder
- 38 CFR 3.304(f)(3), PTSD based on fear of hostile military activity
- 38 CFR 3.400 and 38 USC 5110, effective dates; 38 CFR 3.155, intent to file
- 38 CFR 3.2501, new and relevant evidence to reopen a previously denied claim
- 38 CFR 4.16 and 38 USC 1114(s), TDIU and housebound SMC
- 38 USC 1110 and 38 USC 1131, basic service connection
- Shedden v. Principi, 381 F.3d 1163 (Fed. Cir. 2004), the three-element test for service connection: a current disability, in-service incurrence or aggravation, and a causal nexus
- VA.gov, Military sexual trauma and disability compensation
- VA.gov, disability compensation eligibility for PTSD and mental health conditions