VA GERD Claims Guide
Gastroesophageal reflux disease (GERD) is one of the most commonly claimed digestive conditions, and the rules for rating it changed substantially in 2024. As of the March 2024 digestive reorganization, GERD has its own diagnostic code, diagnostic code 7206, rated on an esophageal stricture and dysphagia scheme rather than on heartburn severity. Before that change, GERD was rated by analogy under the old hiatal hernia code. The service-connection paths range from direct in-service onset to secondary connections, most notably GERD caused by medication taken for a service-connected mental-health condition and GERD linked to sleep apnea. This guide covers all of it in plain language, with the current rating numbers, the whole filing and appeals path, and what we found in the Board's published decisions.
 One-page guide: GERD Claim in One Page
Five-part visual guide to GERD claims covering diagnosis, direct and secondary service connection, dysphagia and stricture evidence, current DC 7206 ratings, and a filing checklist. Opens the full-size chart, free to save or print.
One-page guide: GERD Claim in One Page
Five-part visual guide to GERD claims covering diagnosis, direct and secondary service connection, dysphagia and stricture evidence, current DC 7206 ratings, and a filing checklist. Opens the full-size chart, free to save or print.
Overview
GERD is rated under DC 7206 within 38 CFR 4.114. GERD claims work a bit differently from many conditions: the easiest path to a grant is often not proving the reflux started in service, but showing it was caused or worsened by a condition VA already covers. In a review of the Board's published decisions on GERD, service-connection grants, direct and secondary combined, were common, but so were denials for a missing in-service link, no current diagnosis, or a missed exam; a separate share of cases were not about winning coverage at all, but disputes over the rating percentage or the effective date once GERD was already service connected. This guide walks the whole path: how service connection works, the direct and secondary pathways, what evidence wins, why claims get denied, a checklist before you file, the claims process step by step, how to read your decision letter, and what to do whether you win or you're denied.
What the VA Counts as Gastroesophageal reflux disease (GERD)
GERD is a chronic condition in which stomach acid repeatedly flows back up into the esophagus, the tube that connects the throat to the stomach. The common symptoms are heartburn, regurgitation, chest discomfort, and difficulty or pain when swallowing (called dysphagia). Over time, repeated acid exposure can inflame or narrow the esophagus. That narrowing is called an esophageal stricture, and as you will see below, the current VA rating turns heavily on whether a stricture is documented.
For VA purposes, GERD is now rated under 38 CFR 4.114, diagnostic code 7206, which is specifically titled "Gastroesophageal reflux disease." That code does not stop at GERD. Note 3 to DC 7206 states that it applies to a broad family of esophageal conditions, including esophagitis (mechanical or chemical), Mallory Weiss syndrome from caustic ingestion, drug-induced or infectious esophagitis, idiopathic eosinophilic or lymphocytic esophagitis, esophagitis from radiation therapy, esophagitis due to peptic stricture, and any esophageal condition that requires treatment with sclerotherapy.
GERD (the reflux itself)
Chronic acid reflux into the esophagus. Rated under DC 7206 on a scale built around documented esophageal stricture, dysphagia, the number of dilatation procedures per year, and the most severe complications.
Esophageal stricture (DC 7203)
A narrowing of the esophagus. Rated under the closely related DC 7203, which carries a nearly identical 0/10/30/50/80 ladder and the same documentation notes. Several other esophagus codes now point to DC 7203.
 One-page guide: Symptoms Recorded in Granted GERD Decisions
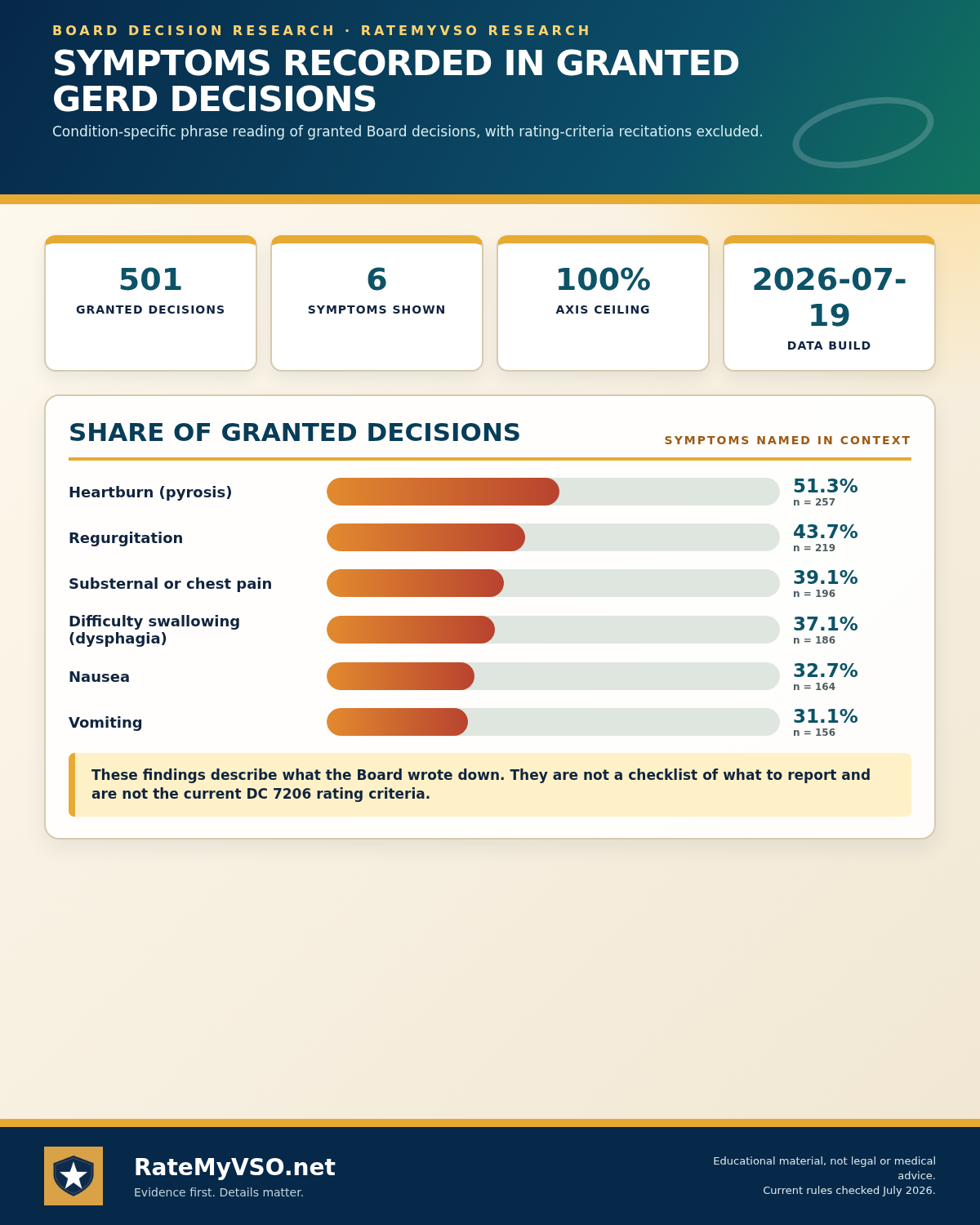
Bar chart of the symptoms most often recorded across 501 granted GERD Board decisions, with rating-criteria recitations excluded. Opens the full-size chart, free to save or print.
One-page guide: Symptoms Recorded in Granted GERD Decisions
Bar chart of the symptoms most often recorded across 501 granted GERD Board decisions, with rating-criteria recitations excluded. Opens the full-size chart, free to save or print.
Symptoms Recorded in Granted GERD Decisions
We analyzed 501 granted Board decisions involving gerd for symptoms named in sentences about the condition (rating-criteria recitations excluded). Descriptive of the published record, what the Board wrote down, not a checklist of what to report.
Detected by phrase-reading the decision text with condition-specific vocabularies. Source: Board of Veterans' Appeals decisions, RateMyVSO analysis.
ICD-10 Diagnosis Codes
The ICD-10 diagnosis codes most commonly used for DC 7206, Gastroesophageal reflux disease (the kind on your medical records, decision letter, or C&P exam report). VA rates the disability and its residuals, not the diagnosis itself, so coding can vary.
How Service Connection Works, At a High Level
Before the specific pathways below, it helps to understand the three things every GERD claim ultimately has to show. This is the same basic test that applies to any VA disability claim, just applied to this condition.
- A current diagnosis. You need GERD, or acid reflux, diagnosed now or at some point during your claim. Without a current diagnosis there is nothing to connect to service.
- An in-service event, or a service-connected condition behind it. Either your reflux began during service (shown by records or credible symptoms), or it was caused or worsened by a disability VA already covers, such as a mental-health condition, IBS, or medication taken for a service-connected joint.
- A medical nexus. A medical opinion connecting your GERD to that in-service cause or service-connected condition, and the opinion carries far more weight when it explains its reasoning rather than stating a bare conclusion.
How Gastroesophageal reflux disease (GERD) Gets Service Connected
Direct service connection
Direct service connection requires the three standard elements: a current GERD diagnosis, an in-service event or onset (for example, documented reflux, dyspepsia, or treatment during service), and a medical nexus linking the two. The framework a direct claim is decided under is described in M21-1, Part V, Subpart i, Chapter 1, Section A. In the Board's published decisions, the missing nexus is by far the most common reason a direct GERD service-connection claim is denied. Continuity of symptoms, in-service records of reflux or stomach trouble plus a steady history of symptoms since, is one of the stronger forms of direct evidence, alongside lay and buddy statements describing what a family member or fellow servicemember personally observed. See 38 CFR 3.303.
Presumptive service connection
There is no toxic-exposure presumptive for GERD itself. GERD is a structural and functional reflux condition with a known cause, so it is not on any Agent Orange, burn pit, or PACT Act presumptive list, and it is not one of the eight Camp Lejeune presumptive conditions. One narrow, adjacent pathway exists for Persian Gulf War veterans: the VA presumes service connection for qualifying chronic, medically unexplained "functional gastrointestinal disorders," a group the VA defines to include irritable bowel syndrome, functional dyspepsia, and functional abdominal pain syndrome, that are at least 10 percent disabling. The current presumptive window runs through December 31, 2026. That pathway covers functional GI disorders without structural change, not a diagnosed structural GERD or esophageal stricture, so it is adjacent rather than a GERD presumptive. See the VA's Gulf War medically unexplained illness page and the presumptive-period extension notice.
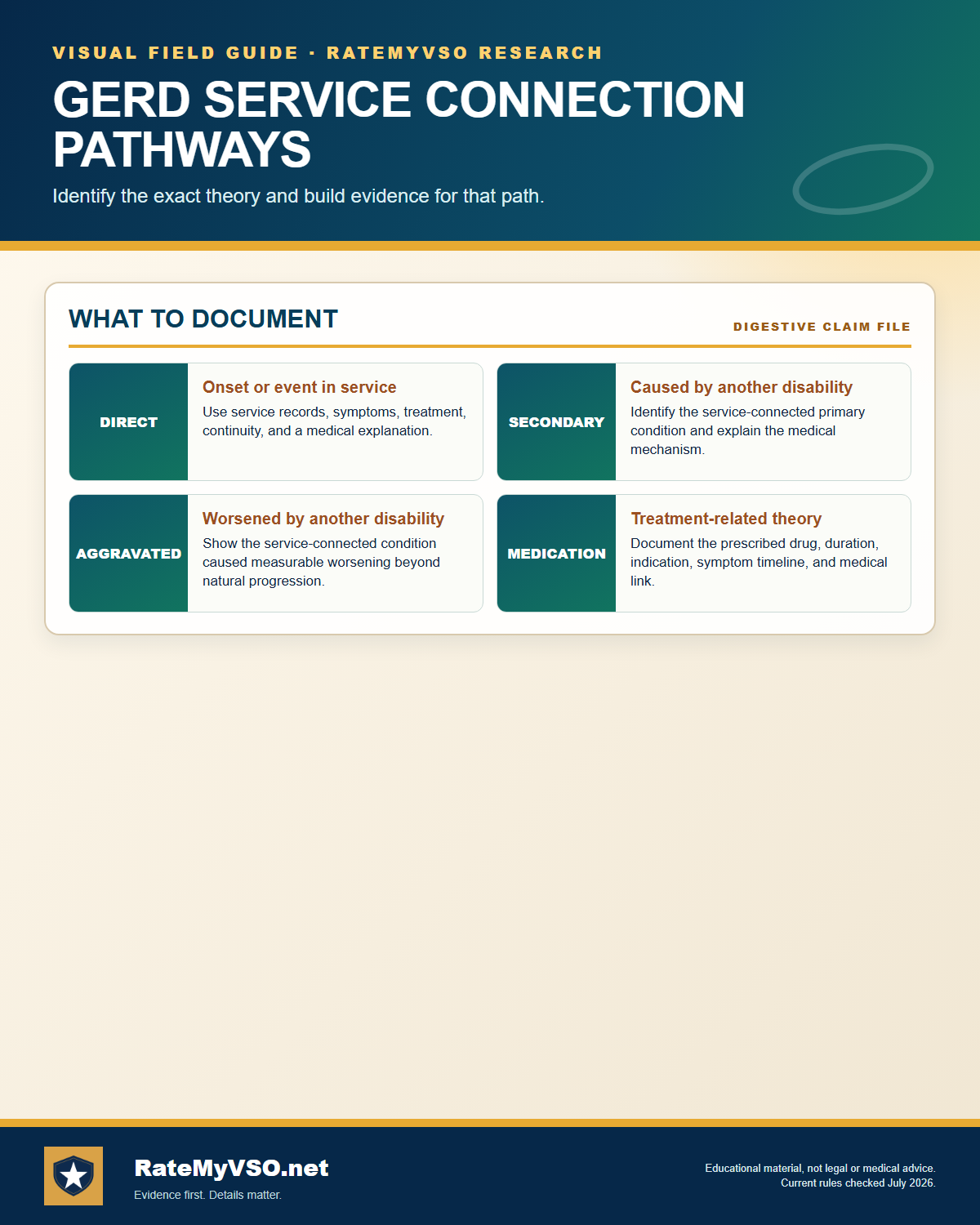
Established secondary pathways for GERD include:
Secondary to a service-connected mental-health condition (medication side effects)
This is one of the strongest and most common winning theories for GERD. Many medications used to treat service-connected mental-health conditions can cause or worsen acid reflux as a side effect. Under 38 CFR 3.310, a secondary claim requires a current GERD diagnosis and a medical nexus opinion stating that the service-connected condition, or its treatment, caused or aggravated the GERD. We found GERD claimed secondary to several mental-health conditions in the Board's published decisions, including psychotic disorders, generalized anxiety disorder, obsessive-compulsive disorder, major depressive disorder, and unspecified depressive disorder. One recognized mechanism is the effect anxiety and related conditions can have on the brain-gut connection. See the PTSD claims guide and nexus letters.
Secondary to obstructive sleep apnea
Sleep apnea is the standout secondary pathway for GERD in the published data. The mechanics are well documented: the pressure changes and arousals of obstructive sleep apnea can promote nighttime acid reflux. In the Board's published decisions, GERD claimed secondary to sleep apnea has been one of the strongest GERD secondary pathways. A nexus opinion linking the service-connected sleep apnea to the GERD is the key evidence under 38 CFR 3.310. See the Sleep Apnea Claims Guide.
Secondary to, or aggravated by, service-connected IBS
Irritable bowel syndrome and GERD are both digestive conditions that can interact. In the Board's published decisions, GERD has been granted as aggravated by a service-connected IBS, supported by a treating gastroenterologist's opinion connecting the two. See the IBS and IBD Claims Guide.
Secondary to long-term pain medication (NSAIDs)
Long-term use of anti-inflammatory pain medication (NSAIDs), often prescribed for a service-connected knee, back, or other joint condition, is a recognized mechanism for causing or worsening GERD. This is an intermediate-step chain under 38 CFR 3.310: the service-connected condition leads to the prescribed medication, and the medication causes or aggravates the reflux. A nexus opinion should name the specific medication, the duration of use, and the mechanism.
Secondary to other service-connected conditions
The published data also surface GERD claimed secondary to service-connected arthritis and to a service-connected peptic ulcer condition. As with every secondary path, the deciding document is a medical opinion that explains the biological link and connects the service-connected primary condition to the GERD. See secondary conditions.
What VA Looks For: Tests, Records, and Diagnostic Codes
Whether you're filing directly or secondary to another condition, the record VA actually reviews centers on a small set of documents and data points.
- The diagnosis itself: a current GERD diagnosis from a VA or private exam, ideally supported by one of the imaging methods discussed under Diagnostic Tests below.
- Service treatment records: any documentation of heartburn, reflux, vomiting, or stomach medication during service, or a steady history of symptoms since discharge.
- The diagnostic codes involved: DC 7206 for GERD itself, plus whatever code applies to the condition you're connecting it to, for example a service-connected psychiatric disorder, DC 7319 (IBS), or the code for a service-connected knee or back condition behind a long-term pain medication.
- The actual form the examiner fills out: the esophageal-conditions Disability Benefits Questionnaire (DBQ), discussed later in this guide.
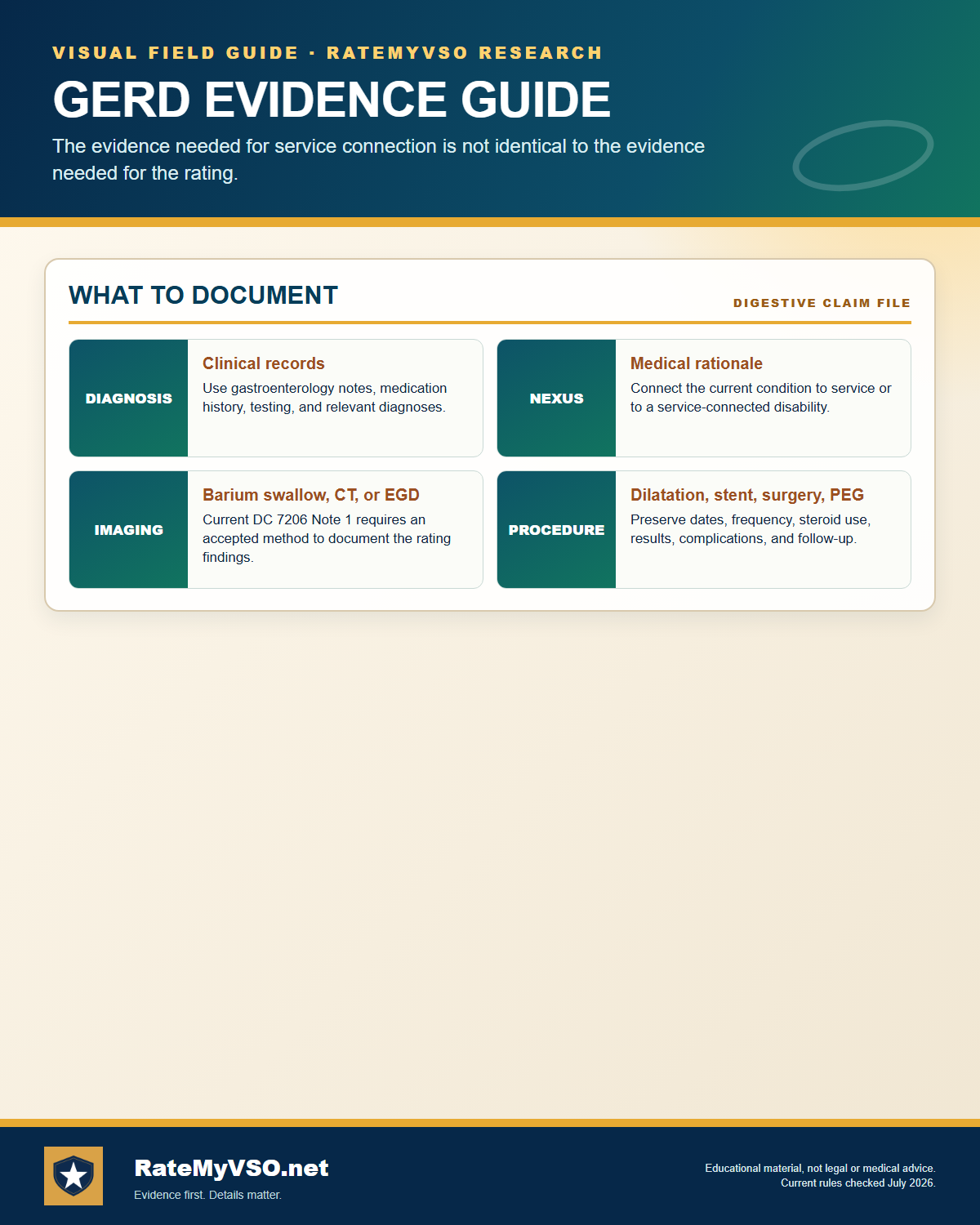 One-page guide: GERD Evidence Guide
Diagnosis, nexus, accepted imaging, and procedure evidence. Opens the full-size chart, free to save or print.
One-page guide: GERD Evidence Guide
Diagnosis, nexus, accepted imaging, and procedure evidence. Opens the full-size chart, free to save or print.
Evidence That Wins These Claims
We analyzed the Board's published decisions and found a private medical opinion is the highest-yield evidence for these claims:
For the rating level (as opposed to service connection), the deciding evidence is the imaging and procedure record: a barium swallow, CT, or EGD documenting the stricture (per Note 1), plus dilatation procedure notes showing how many dilatations occurred per year and whether any used steroids or involved a stent. See the DBQ guide.
Evidence Checklist
- Current diagnosis: a GERD (or acid reflux) diagnosis in your VA or private medical records, ideally supported by a barium swallow, CT, or EGD.
- In-service records or continuity of symptoms: for a direct claim, records showing reflux, stomach trouble, vomiting, or related medication during service, plus a steady history of symptoms since. This continuity-of-symptoms evidence, under 38 CFR 3.303, has supported direct grants where in-service records documented reflux symptoms and treatment well before the current claim.
- Lay and buddy statements: you don't need a doctor to describe what you felt. First-person and family statements describing frequent heartburn, regurgitation, or vomiting, especially during and shortly after service, have supported grants alongside the medical evidence. See the Buddy & Lay Statements Guide.
- A reasoned medical nexus opinion: the clearest path to a grant is an opinion that explains how the connection works, cites supporting medical literature applied to your own facts, and directly addresses each service-connected condition you're claiming as the source, rather than a bare conclusion.
- The diagnostic codes involved: DC 7206 for the GERD itself, plus the code for whatever condition you're connecting it to (a mental-health code, DC 7319 for IBS, or the code covering the joint condition behind a long-term medication).
Evidence Cited in Published GERD Decisions
We analyzed 6,701 published Board decisions involving gerd for condition-specific evidence, counting only case-specific mentions (boilerplate recitations excluded). "Favorable" is the share of decisions citing that evidence where every issue was granted or the outcome was mixed; the baseline across all these decisions is 62.5%. Evidence appearing in a decision does not mean it decided the case. Descriptive of the published record, not a prediction.
Detected by phrase-reading the decision text with condition-specific vocabularies. Source: Board of Veterans' Appeals decisions, RateMyVSO analysis.
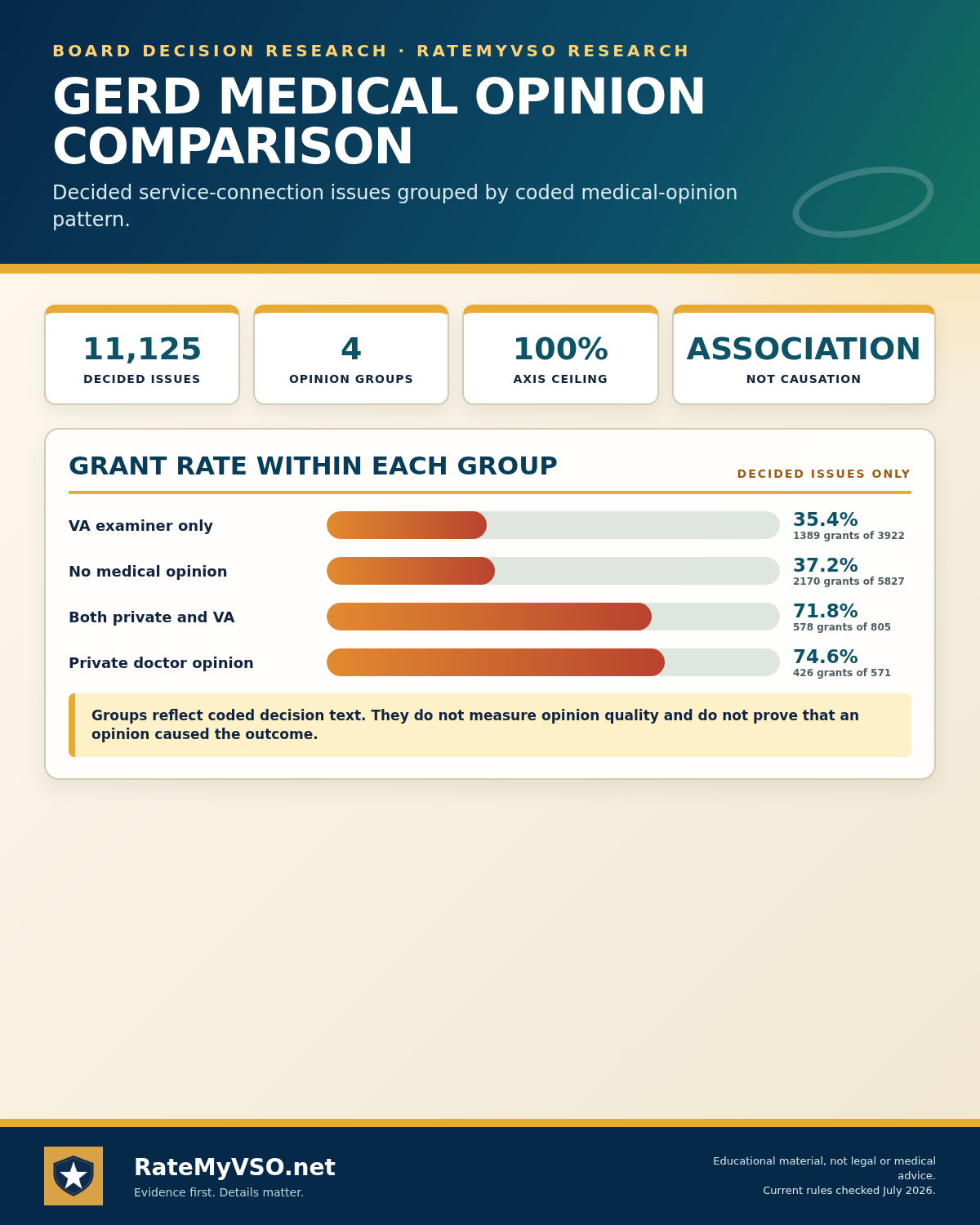 One-page guide: GERD Medical Opinion Comparison
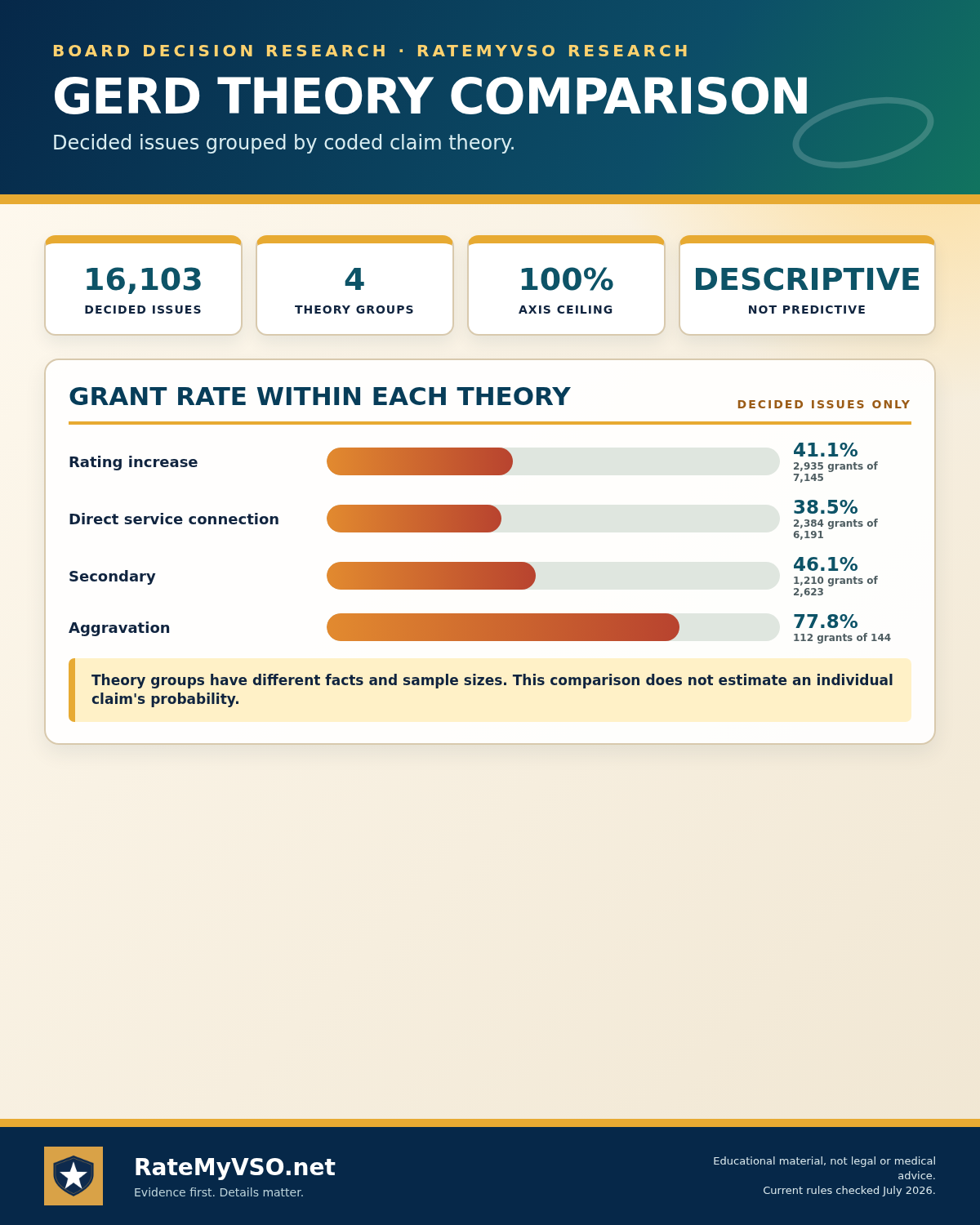
GERD: descriptive grant rates by coded opinion group across 11,125 decided issues. Opens the full-size chart, free to save or print.
One-page guide: GERD Medical Opinion Comparison
GERD: descriptive grant rates by coded opinion group across 11,125 decided issues. Opens the full-size chart, free to save or print.
Why These Claims Get Denied
Beyond the general "no nexus" and "no current diagnosis" reasons covered above, a few specific denial patterns show up often enough in the Board's published decisions to call out on their own.
- No current diagnosis in the file. Without a GERD or acid reflux diagnosis at some point during the claim, there is nothing to connect to service, regardless of how the veteran describes their symptoms.
- The veteran's own belief about the cause, without a doctor's opinion behind it. A veteran is competent to report symptoms, but the medical cause of GERD is treated as a question requiring medical training. Claims have failed where the only link to service was the veteran's personal opinion, without a supporting medical nexus.
- A missed VA examination. If VA schedules an exam and the veteran doesn't report without good cause, VA can decide the claim on the record as it stands under 38 CFR 3.655, which has led to denials on its own.
- A long gap between service and the first documented sign of GERD, with nothing to fill it. A first diagnosis years or decades after discharge, with no in-service record and no lay evidence of ongoing symptoms in between, is treated as evidence against the claim.
- A vague exposure claim with no medical opinion behind it. Attributing GERD generally to fuel, chemicals, or food during service, without a medical opinion tying a specific mechanism to the veteran's facts, is a weak claim on its own. A general article about an exposure, unconnected to the veteran's own record, has been rejected as too generic to help.
- Leaning on the Gulf War presumption. GERD is treated as a structural disease, not an unexplained illness, so the Persian Gulf War presumptive pathway does not reach it. A claim resting only on that presumption, with no direct or secondary theory behind it, will not succeed on the presumption alone.
- Confusing a rating or effective-date dispute with a service-connection denial. Being service connected for GERD is a separate question from the percentage you're rated at or the date your award starts. Some cases that look like a "GERD denial" are really a fight over the rating level or an earlier effective date for a GERD that is already service connected.
 One-page guide: GERD Board Denial Reasons
4,675 classified GERD service-connection denials split by the missing element, with the three required direct-claim elements. Opens the full-size chart, free to save or print.
One-page guide: GERD Board Denial Reasons
4,675 classified GERD service-connection denials split by the missing element, with the three required direct-claim elements. Opens the full-size chart, free to save or print.
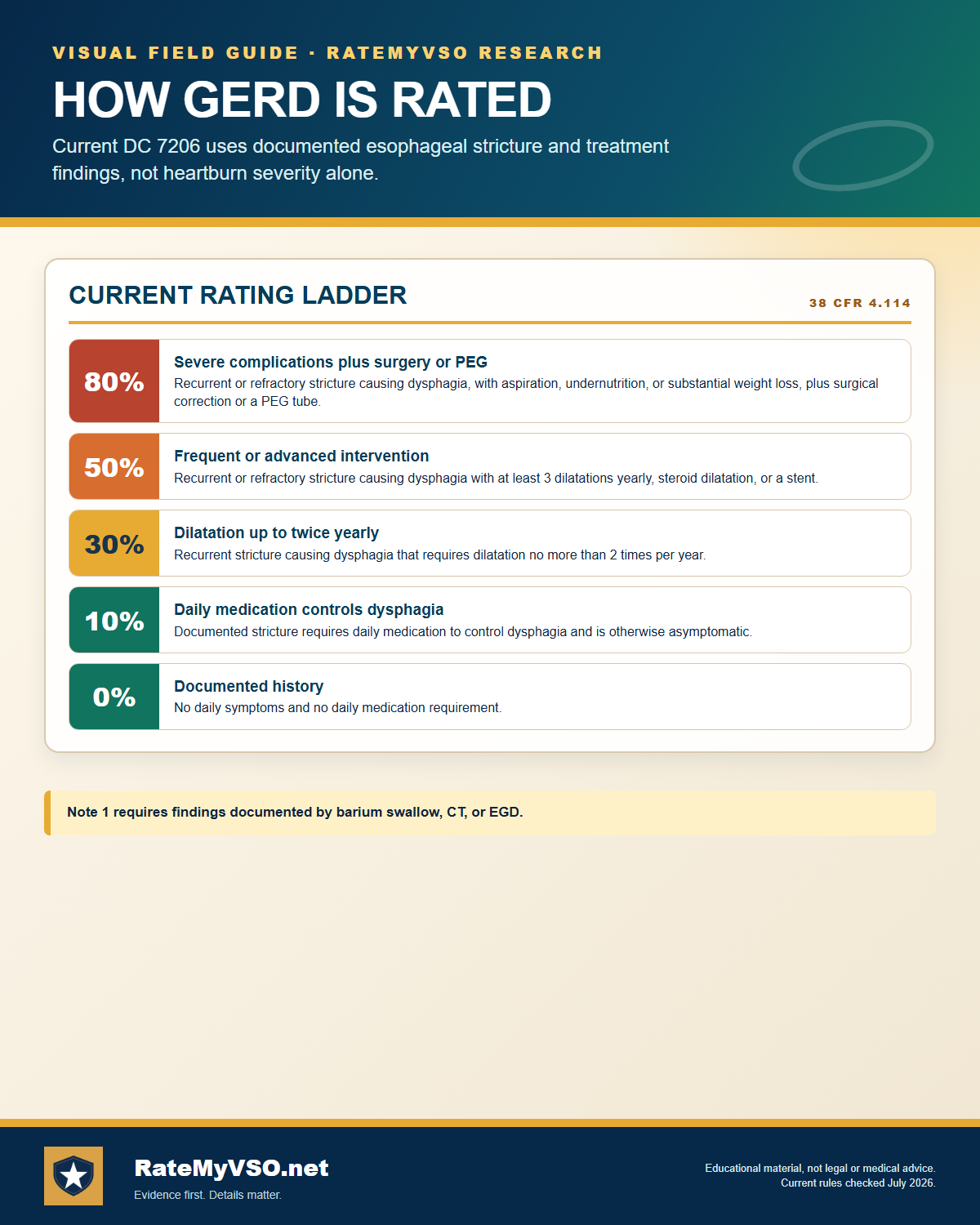
DC 7206 Rating Levels
The full current title in the schedule is "Gastroesophageal reflux disease." Both GERD and the closely related esophageal stricture code (DC 7203) use the same five-step ladder. The rating is driven by documented structural findings and treatment, not by symptom severity alone. Here are the criteria, taken verbatim from 38 CFR 4.114.
Go deeper: open the full GERD breakdown- What the VA measures at your C&P exam
- Evidence that has won at the Board
- Inside the rater's playbook: grant, denial, and remand rates
- Secondary condition map
80 percent is the maximum schedular rating for GERD. There is no 60 percent and no 100 percent level under DC 7206. The plain-language version of each row is below.
| Rating | In plain language |
|---|---|
| 0% | A documented history of the condition, but no daily symptoms and no need for daily medication. |
| 10% | A documented stricture that is controlled by daily medication and is otherwise without symptoms. |
| 30% | A documented recurrent stricture causing dysphagia that requires dilatation no more than two times per year. |
| 50% | A documented recurrent or refractory stricture causing dysphagia that requires dilatation three or more times per year, or steroid dilatation at least once a year, or an esophageal stent. |
| 80% | A documented recurrent or refractory stricture causing dysphagia, with aspiration, undernutrition, and/or substantial weight loss, plus either surgical correction or a PEG (feeding) tube. |
The other notes from the regulation:
- Note 1: Findings must be documented by barium swallow, computerized tomography, or esophagogastroduodenoscopy.
- Note 2: Non-gastrointestinal complications of procedures should be rated under the appropriate system.
- Note 3: This code applies to a broad list of esophageal conditions, including esophagitis (mechanical or chemical), Mallory Weiss syndrome from caustic ingestion, drug-induced or infectious esophagitis, idiopathic eosinophilic or lymphocytic esophagitis, esophagitis from radiation therapy, esophagitis due to peptic stricture, and any esophageal condition that requires treatment with sclerotherapy.
- Note 4: "Recurrent" esophageal stricture means the inability to maintain target esophageal diameter beyond 4 weeks after the target diameter has been achieved.
- Note 5: "Refractory" esophageal stricture means the inability to achieve target esophageal diameter despite receiving no fewer than 5 dilatation sessions performed at 2-week intervals.
The "substantial weight loss" used in the 80 percent row is defined at 38 CFR 4.112(a) as an involuntary loss greater than 20 percent of baseline weight, sustained for three months, with diminished quality of self-care or work tasks.
Pyramiding and Rating Separately
The VA's pyramiding rules prevent paying twice for the same symptoms. The digestive schedule has a specific anti-combining instruction at 38 CFR 4.114. It directs that ratings under a listed group of digestive codes (diagnostic codes 7301 through 7329 inclusive, 7331, 7342, 7345 through 7350 inclusive, 7352, and 7355 through 7357 inclusive) are not combined with each other. Instead, when more than one of those ratings would be warranted, the VA assigns a single evaluation under the code that reflects the predominant disability picture, and elevates it one step if the overall severity warrants it.
What still applies to every claim is the general pyramiding rule at 38 CFR 4.14: the same manifestation cannot be evaluated twice under two different diagnoses. The two codes are built around different findings, GERD on documented stricture and dysphagia, IBS on abdominal pain related to defecation, so a record that documents genuinely separate symptoms can support separate ratings. Where the file instead describes one common set of abdominal complaints, 38 CFR 4.113 explains why coexisting abdominal conditions often cannot be split apart without pyramiding. That is a question about what your records show, not a rule that automatically collapses GERD and IBS into one rating.
Where GERD produces a complication outside the digestive system, Note 2 to DC 7206 directs that the non-gastrointestinal complication be rated under the appropriate body system rather than folded into the GERD rating.
Common Mistakes
These are the recurring errors the published decisions and the regulation history surface for GERD claims.
- Relying on an outdated guide: assuming GERD is still rated under DC 7346 on the old 10/30/60 percent pyrosis and epigastric-distress scale. Since the May 19, 2024 reorganization (89 FR 19743), GERD is rated under DC 7206, and DC 7346 simply says "rate as DC 7203," so the old 60 percent hiatal-hernia ceiling no longer exists.
- Expecting a 60 or 100 percent level: the current DC 7206 ladder tops out at 80 percent (0/10/30/50/80). There is no 60 percent and no 100 percent schedular rating for GERD.
- Assuming severe daily heartburn alone yields a high rating: the 30, 50, and 80 percent levels are built around documented esophageal stricture, dysphagia, dilatation frequency, stent or PEG placement, aspiration, and substantial weight loss. Symptom severity without those structural or treatment findings generally caps the rating near 10 percent.
- Not having the condition documented by an accepted imaging method: DC 7206 Note 1 requires findings shown by barium swallow, CT, or EGD. Claims resting on symptom reports alone often fall short of the higher rows.
- Filing direct-only and omitting a nexus opinion: "no nexus" is the single biggest denial driver for GERD, and grant rates are much higher when a private nexus letter is in the file.
- Overlooking the secondary pathway: the published data show GERD caused or aggravated by medication taken for a service-connected mental-health condition, or claimed alongside sleep apnea or IBS, is often a stronger route than direct service connection.
- Confusing the Gulf War functional-GI presumptive with structural GERD: that presumption covers medically unexplained functional disorders (irritable bowel syndrome, functional dyspepsia, functional abdominal pain), not a diagnosed esophageal or reflux condition with a known cause.
Pitfalls and Procedural Mistakes
Distinct from the substantive reasons claims get denied above, these are process mistakes that can sink an otherwise winnable file.
- Skipping a scheduled C&P exam. A missed exam without good cause can result in VA deciding the claim on the existing record, which is rarely the veteran's strongest evidence.
- Letting your onset story shift between statements. If the account of when symptoms began changes across forms, exams, and statements, that inconsistency itself becomes a reason to discount the claim.
- Not distinguishing which pathway you're actually arguing. A direct claim and a secondary claim need different evidence, in-service records and continuity of symptoms for direct, versus proof the service-connected condition exists and caused or aggravated the GERD for secondary. Mixing the two without addressing each element can leave gaps a rater has to fill against you.
- Filing overlapping digestive conditions without separating the symptoms. GERD's code is not on the 4.114 do-not-combine list, so a separate rating alongside a condition like IBS is not automatically barred. What sinks these claims is a record describing one undifferentiated set of abdominal complaints, because the same manifestation cannot be counted under two codes. See the pyramiding section below before filing multiple related digestive claims.
- Not challenging an inadequate VA opinion. A VA medical opinion that ignores your lay statements, relies only on the absence of records, rests on an incorrect fact, or applies the wrong legal standard for aggravation can be challenged. Point out the specific flaw in a response or appeal rather than letting the opinion stand unaddressed.
Do's and Don'ts
A condensed version of everything above, in the order it actually matters when you sit down to build your file.
- Get a current GERD diagnosis into your records, from a VA or private exam.
- Look for any service records showing heartburn, reflux, vomiting, or stomach medication.
- Ask whether GERD could be secondary to a condition VA already covers: a mental-health condition, IBS, sleep apnea, or long-term pain medication for a service-connected joint.
- Get a medical nexus opinion that explains its reasoning and, if possible, cites supporting medical literature applied to your own facts.
- Gather lay and buddy statements describing your symptoms during and since service.
- Report for every VA examination that's scheduled.
- If you served in combat, know that your own credible account of in-service onset can be accepted under the combat rule.
- Keep the service-connection question separate from your rating percentage and effective date, know which fight you're in.
- If you were denied before, file a Supplemental Claim with new and relevant evidence rather than starting over.
- Don't assume a diagnosis alone wins the claim, you still need the connection to service.
- Don't rely only on your own opinion about what caused it, causation for GERD is treated as a medical question.
- Don't skip a scheduled VA exam without a good reason.
- Don't let your story about when symptoms began shift between statements and exams.
- Don't count on the Gulf War presumption, GERD is treated as a structural condition, not a presumptive unexplained illness.
- Don't blame a vague exposure (fuel, chemicals, food) without a medical opinion tying it to your specific facts.
- Don't expect a 60 or 100 percent rating, the current DC 7206 ladder tops out at 80 percent.
- Don't confuse a rating or effective-date dispute with a service-connection denial.
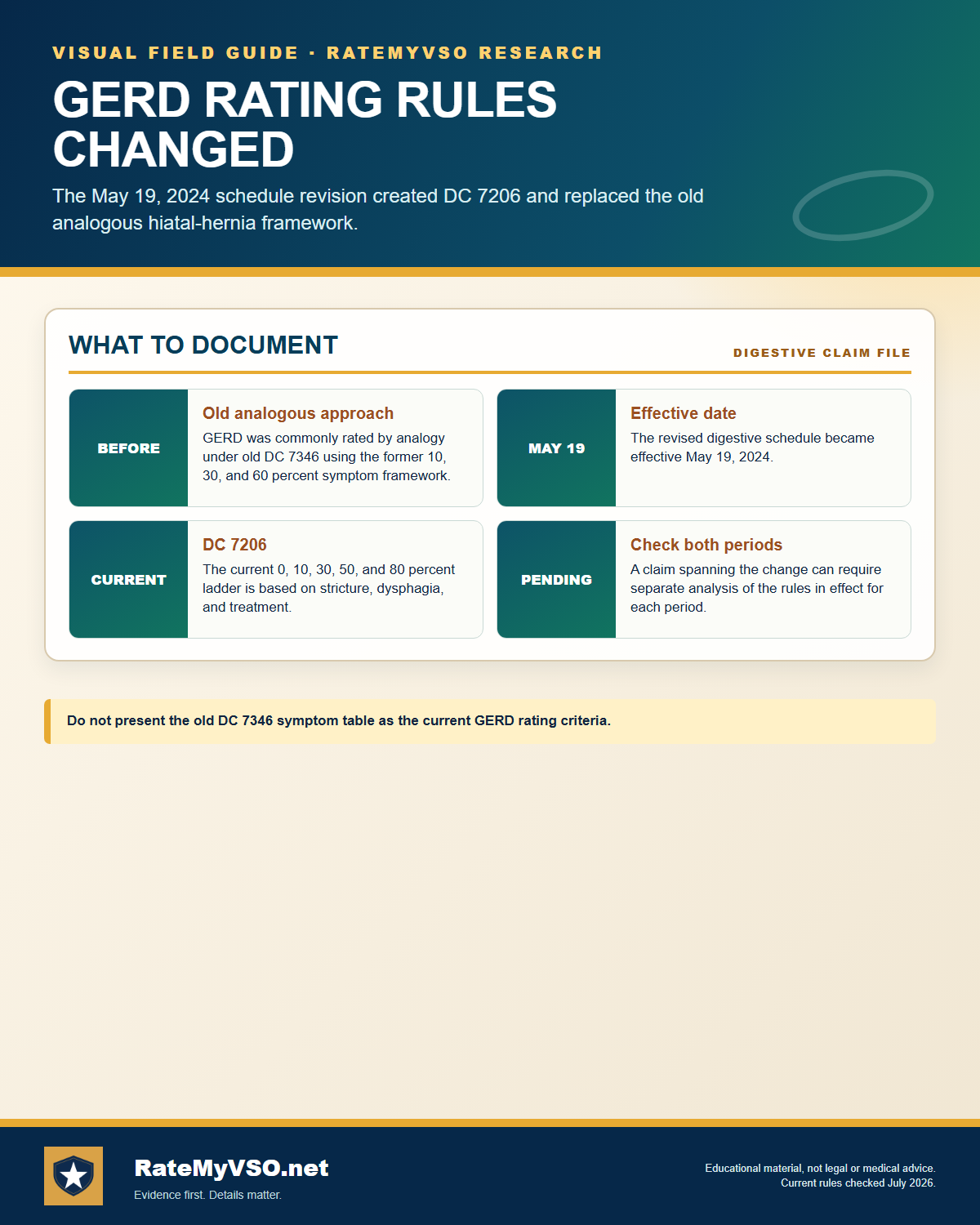
The 2024 Code Transition: From DC 7346 to DC 7206
This is the single most important thing to understand about a GERD claim today, because most older guides on the internet are now out of date.
What changed, in plain language
- Before the 2024 reorganization: GERD was not its own code. Raters evaluated it by analogy, most often under DC 7346 (hiatal hernia), which topped out at 60 percent for symptoms such as persistent pyrosis (heartburn), regurgitation, substernal or arm or shoulder pain, and dysphagia productive of considerable impairment of health.
- After the 2024 reorganization: GERD is DC 7206. The ladder is 0/10/30/50/80, and the criteria are built around documented esophageal stricture, dysphagia, the number of dilatation procedures per year, stent or PEG tube placement, aspiration, and substantial weight loss. The highest available schedular rating is 80 percent.
When a regulation changes, the VA generally applies the version of the rule that is more favorable to the veteran for the period each version was in effect. The VA's own manual guidance and longstanding case law direct raters to consider both the old and new criteria for a claim that was pending across the change, and to use whichever yields the higher evaluation for the relevant time period. In practice this means a claim filed before the May 2024 effective date may still be evaluated under the old DC 7346 criteria for the earlier period, while a claim filed after that date is evaluated under DC 7206. This guide reports what the regulation says. It does not predict which version applies to any individual file.
 One-page guide: GERD Claim Checklist
GERD: eight pre-filing checks. Opens the full-size chart, free to save or print.
One-page guide: GERD Claim Checklist
GERD: eight pre-filing checks. Opens the full-size chart, free to save or print.
Quick Checklist Before You File
Bring these together before you submit anything.
- A current GERD diagnosis in your records, from a VA or private exam.
- Any service records showing heartburn, reflux, vomiting, or stomach medication.
- A list of every service-connected condition that could plausibly connect: mental health, IBS, sleep apnea, or long-term pain medication for a joint condition.
- A medical nexus opinion that explains its reasoning and, where possible, cites supporting medical literature.
- Lay and buddy statements describing your symptoms during and since service.
- Imaging or procedure records (barium swallow, CT, or EGD) if you're also pursuing a specific rating level, not just service connection.
- If you were denied before: new and relevant evidence for a Supplemental Claim, not just a repeat of what was already considered.
For the mechanics of actually submitting the claim, see the Standard Claim Guide and the Fully Developed Claim Guide (filing with all your evidence up front can speed up the decision).
The Claims Process, Step by Step
Once you file, your claim moves through a series of hand-offs. Understanding who does what helps you know who to contact, and what to expect, at each stage.
- You file the claim. Directly with VA, through VA.gov, or with the help of an accredited representative.
- VA acknowledges the claim and assigns it for development. A Veteran Service Representative (VSR) is assigned to gather your service treatment records, VA and private medical records, and any other evidence needed.
- The VSR orders a Compensation & Pension (C&P) exam if one is needed. Most GERD claims involve one, especially secondary claims where a nexus opinion is required.
- The C&P exam is conducted. By a VA clinician or a contracted examiner, who completes the esophageal-conditions Disability Benefits Questionnaire (DBQ) documenting the diagnosis, severity, and, where relevant, a nexus opinion.
- The file goes to a Rating Veteran Service Representative (RVSR), the "rater." The rater reviews the complete file, including the exam results, and decides whether service connection is warranted and at what percentage.
- A senior reviewer may review the decision before it's finalized, depending on the complexity of the claim.
- VA issues the decision letter. This states whether the claim is granted or denied, the rating percentage if granted, and the reasons behind the decision.
- If you disagree, you choose an appeal lane. Higher-Level Review, Supplemental Claim, or a Board appeal, covered later in this guide.
Who's who: VSO vs. VSR vs. Rater vs. C&P Examiner
Your VSO
An accredited representative from a veterans service organization, or an accredited attorney or claims agent. Not a VA employee. Helps you prepare, gather evidence, and file, and can represent you through an appeal. Has no authority to decide your claim.
VSR (Veteran Service Representative)
VA staff who "develops" your claim: requests records, schedules the C&P exam, and assembles the file. Does not decide the rating.
Rater (RVSR)
VA staff who reviews the completed file and makes the actual decision, service connection or denial, and the percentage. This is the person whose judgment the decision letter reflects.
C&P Examiner
A VA clinician or a contracted medical examiner who conducts the exam and completes the DBQ. Documents findings and, where asked, a nexus opinion. Does not decide the claim.
For the full walkthrough of every stage with more detail, see Inside Your Claim and Claim Stages.
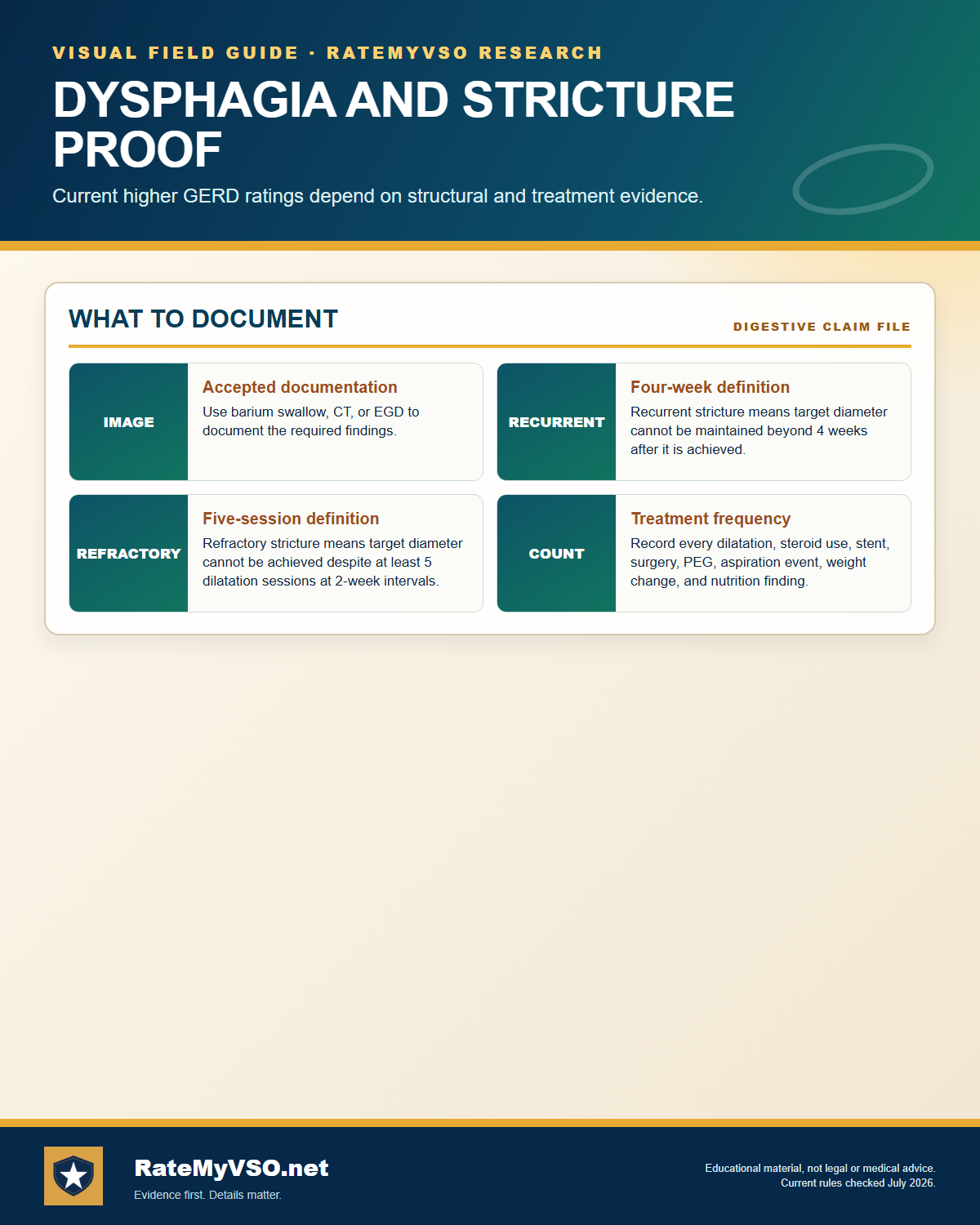 One-page guide: Dysphagia and Stricture Proof
Accepted imaging and current definitions of recurrent and refractory stricture. Opens the full-size chart, free to save or print.
One-page guide: Dysphagia and Stricture Proof
Accepted imaging and current definitions of recurrent and refractory stricture. Opens the full-size chart, free to save or print.
Diagnostic Tests and the DBQ
The primary Disability Benefits Questionnaire for this condition is VA Form 21-0960G-1, "Esophageal Conditions (Including Gastroesophageal Reflux Disease (GERD), Hiatal Hernia and Other Esophageal Disorders)." The questions on that form track the rating criteria, so the underlying tests below are what give the form, and the rater, something to work with. The evaluation framework is described in M21-1, Part V, Subpart iii, Chapter 6, Digestive Disabilities.
- Esophagogastroduodenoscopy (EGD, or upper endoscopy): direct visualization of esophagitis, erosions, strictures, and Barrett's esophagus. One of the three imaging methods DC 7206 Note 1 accepts.
- Barium swallow (esophagram, or upper GI series): accepted under DC 7206 Note 1 to document stricture and dysphagia.
- Computed tomography (CT) of the chest or abdomen: the third imaging method accepted under DC 7206 Note 1.
- Esophageal dilatation records and procedure notes: the count and method of dilatations per year (and any steroid dilatation or stent placement) drive the difference between the 30 and 50 percent levels.
- Documentation of daily medication use: proton pump inhibitors (such as omeprazole, pantoprazole, or lansoprazole) or H2 blockers. Per M21-1, daily medication used to control symptoms supports the 10 percent level even without a separately documented stricture.
- Weight and nutrition records and aspiration findings: needed to assess the 80 percent criteria (aspiration, undernutrition, substantial weight loss under 38 CFR 4.112(a)) and any PEG-tube placement.
- 24-hour esophageal pH monitoring and esophageal manometry: sometimes used clinically to confirm reflux and esophageal motility, supporting the diagnosis.
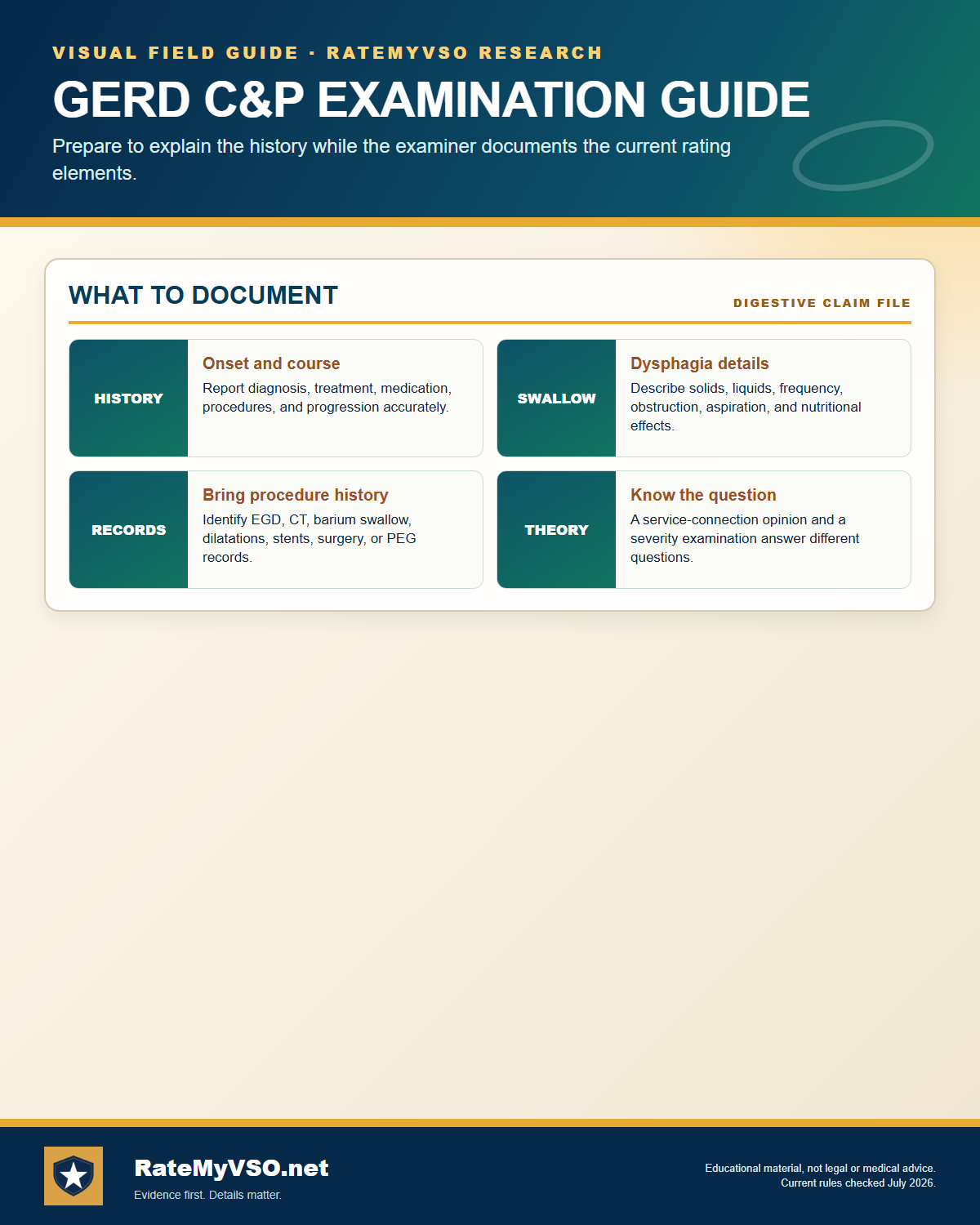 One-page guide: GERD C&P Examination Guide
History, dysphagia, procedure records, and examination purpose. Opens the full-size chart, free to save or print.
One-page guide: GERD C&P Examination Guide
History, dysphagia, procedure records, and examination purpose. Opens the full-size chart, free to save or print.
Your C&P Exam
See the DBQ Guide for how the esophageal-conditions DBQ works in general, including whether a private DBQ completed by your own doctor can be submitted instead of relying solely on a VA exam.
Before your C&P exam, bring a clear, specific account of your symptoms, focus on how the condition affects your daily function on your worst days, not just an average day. Be consistent with what's already in your medical records and prior statements, since an inconsistent onset story is one of the pitfalls covered above. For a full walkthrough of what to expect and how to prepare, see the C&P Exam Prep Guide.
Reading Your Decision Letter, and What to Do If Denied
Your decision letter has two parts: a narrative section explaining the reasoning (often called "reasons and bases"), and a codesheet showing the actual rating percentage, the effective date, and the diagnostic code used. See the Reading Your Decision Letter Guide for how to find and interpret each part, or use the Letter Interpreter tool to upload your own letter and get a plain-English breakdown.
If your claim is denied, or the rating is lower than you expected, you have three main lanes:
- Supplemental Claim: refile with new and relevant evidence, such as a new nexus opinion or updated imaging. See Supplemental Claim Guide.
- Higher-Level Review (HLR): a senior reviewer looks at the same evidence again for a difference of opinion, no new evidence is added. See HLR Guide.
- Board Appeal: your case goes to a Veterans Law Judge at the Board of Veterans' Appeals, with options for a direct review, an evidence docket, or a hearing. See Board Appeal Guide.
Not sure which lane fits your situation? See the Appeals decision guide for a side-by-side comparison of all three.
After You Win: Maintaining Your Rating and Getting the Right Start Date
A grant is not always the end of the story. Keep your treatment consistent, continued follow-up and records showing ongoing symptoms and management, protects you if VA schedules a future reexamination. Not every rating gets reexamined; understand when a rating becomes protected from future review and what to do if VA proposes to reduce it. See Protect Your Rating and Future Reexaminations for the specifics.
Two details specific to GERD are worth knowing once you're already service connected. First, DC 7206 itself references medication: its 10 percent level covers a documented stricture requiring daily medication to control dysphagia, and its 0 percent level covers a history without daily symptoms or daily medication. That is different from a code that says nothing about treatment, where VA generally must evaluate symptoms as they would be without the relief medication provides (Jones v. Shinseki, 26 Vet. App. 56 (2012)). Either way, describe your symptoms as they are day to day, not just how you feel while treated. Second, GERD's code is not on the 4.114 do-not-combine list, so a rating alongside another digestive condition like IBS is not automatically barred; what cannot happen is the same symptom being counted under both, see Pyramiding above. If your GERD worsens after the initial grant, for example progressing to require dilatation more often or a newly documented stricture, you can file for an increased rating. See the Rating Increase Guide.
For the effective date of your award: it's generally the date VA received your claim or the date the condition arose, whichever is later, and it can't be earlier than the day after you left service. Filing an intent to file can preserve an earlier date only if you complete the claim within one year. See the Reading Your Decision Letter Guide for more on effective dates.
Common Secondary Conditions
Secondary conditions run in two directions: conditions that can cause GERD, and conditions that GERD can in turn cause. The Board's published decisions catalogue both directions, and the grant rates differ sharply by pathway.
Conditions that can cause GERD (GERD as the secondary)
When GERD is claimed as secondary to a service-connected primary condition, each bar is the published BVA grant rate, with the number of decisions below it. This is the "ways to connect via another condition" list:
(All figures are grant rates from published BVA decisions, secondary-claim dataset. The mental-health pathways generally reflect medication side effects rather than the mental condition itself.)
Conditions GERD can cause (GERD as the primary)
GERD is itself a recognized cause of downstream secondary claims. We found each bar is the published BVA grant rate for a condition claimed secondary to GERD, in other words, conditions secondary to GERD once GERD itself is already service connected:
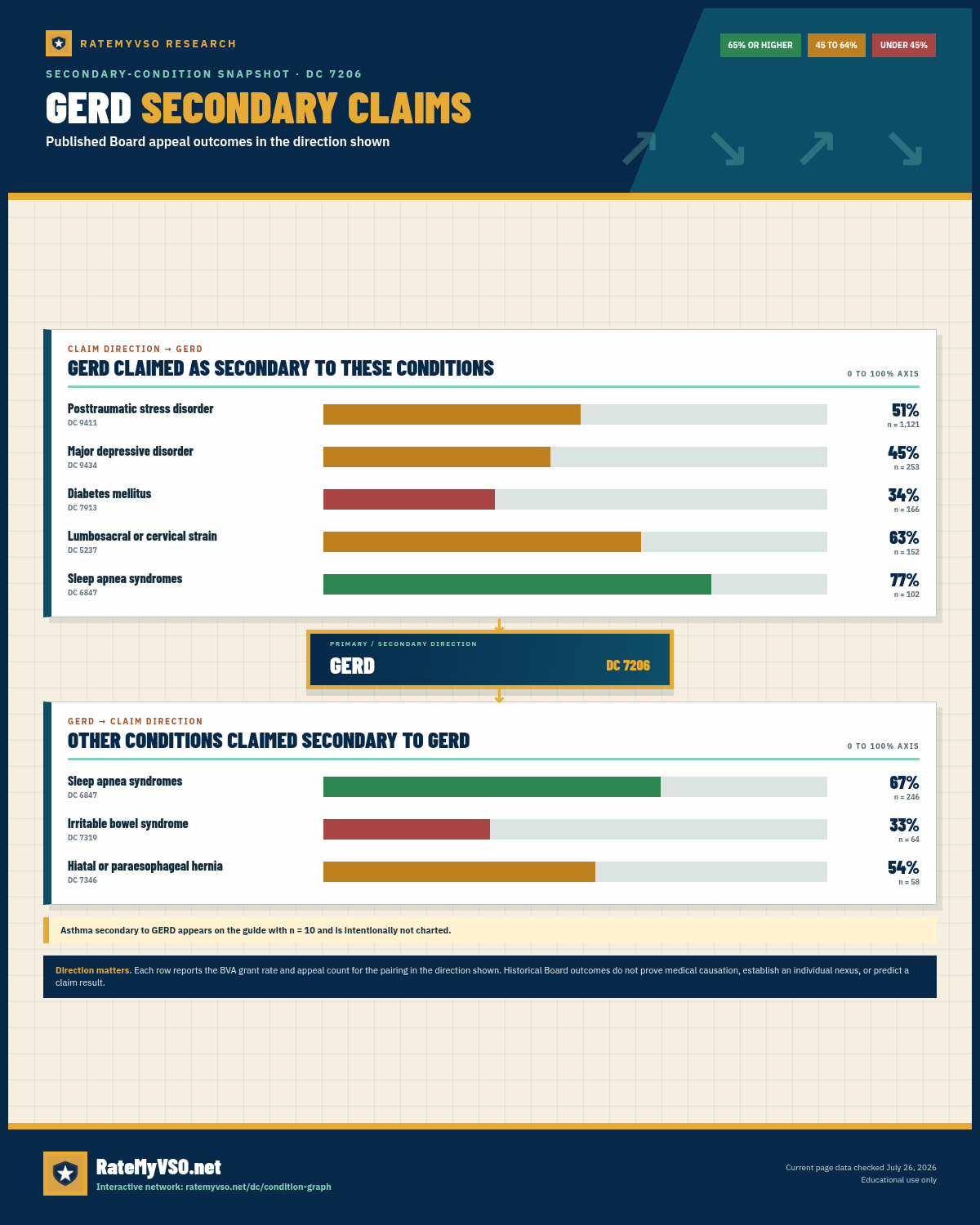 One-page guide: GERD Secondary-Claim Snapshot
Two-direction secondary-claim snapshot for GERD, showing BVA grant rates and appeal counts for conditions claimed toward and away from GERD. Opens the full-size chart, free to save or print.
One-page guide: GERD Secondary-Claim Snapshot
Two-direction secondary-claim snapshot for GERD, showing BVA grant rates and appeal counts for conditions claimed toward and away from GERD. Opens the full-size chart, free to save or print.
Asthma is also claimed secondary to GERD, but on a very small sample (n = 10), so it is not charted here. All figures are from published BVA decisions, secondary-claim dataset.
Board Grants, Dissected
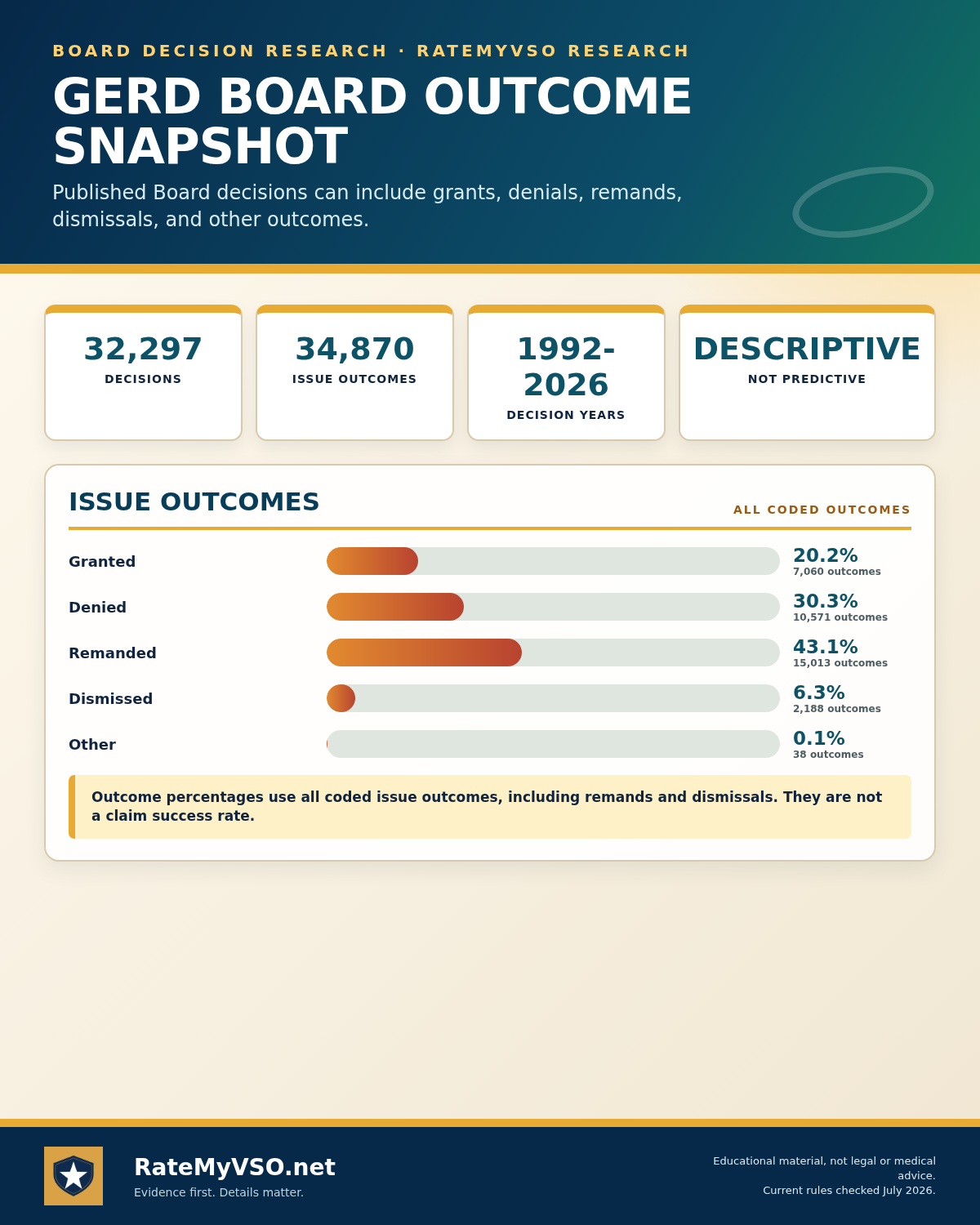 One-page guide: GERD Board Outcome Snapshot
GERD: distribution of coded Board issue outcomes across 34,870 coded issues from 32,297 decisions. Opens the full-size chart, free to save or print.
One-page guide: GERD Board Outcome Snapshot
GERD: distribution of coded Board issue outcomes across 34,870 coded issues from 32,297 decisions. Opens the full-size chart, free to save or print.
Quick Reference Tables
Secondary Connection Pathways
| Primary Condition | Mechanism | Evidence Needed |
|---|---|---|
| Mental-health condition (psychiatric disorder, anxiety, depression) | Medication side effects; effect on the brain-gut connection | Nexus opinion naming the condition or medication and explaining the mechanism |
| Sleep apnea (DC 6847) | Pressure changes and arousals promoting nighttime acid reflux | Nexus opinion linking the service-connected sleep apnea to the GERD |
| IBS (DC 7319) | Interaction between the two digestive conditions | Gastroenterologist opinion connecting the two |
| Long-term NSAID use for a joint condition | Medication causing or aggravating reflux | Nexus opinion naming the medication, duration, and mechanism |
| Arthritis / peptic ulcer | Case-specific mechanism | Medical opinion explaining the biological link |
From Filing to Decision: Who Does What
| Role | Does | Decides your rating? |
|---|---|---|
| VSO / accredited representative | Helps prepare, gather evidence, and file; represents you on appeal | No |
| VSR | Develops the claim: orders records and the C&P exam | No |
| C&P Examiner | Conducts the exam, completes the DBQ, may give a nexus opinion | No / but has a strong impact |
| Rater (RVSR) | Reviews the full file and decides service connection and percentage | Yes |
Frequently Asked Questions
Is GERD still rated under DC 7346 (hiatal hernia)?
What is the highest rating I can get for GERD?
My heartburn is severe and daily. Why might my rating still be low?
Can GERD be service connected as secondary to my mental-health condition?
Is there a presumptive path for GERD?
Which evidence shows up most often in granted GERD decisions?
What if I served in combat and my records don't mention GERD?
Related Tools and Guides
Sources
- 38 CFR 4.114, DC 7206, gastroesophageal reflux disease (digestive schedule)
- 38 CFR 3.303, service connection, including continuity of symptoms; 38 CFR 3.303(d), service connection for a disease diagnosed after service
- 38 CFR 3.310, secondary service connection, caused or aggravated
- 38 CFR 3.102, benefit of the doubt; 38 USC 5107(b), benefit of the doubt
- 38 CFR 3.317, Persian Gulf War presumptive service connection; 38 USC 1117, Persian Gulf War qualifying chronic disability
- 38 CFR 3.301, line of duty and willful misconduct
- 38 CFR 4.113, digestive diseases rated together (no pyramiding)
- 38 CFR 3.400, effective dates; 38 CFR 3.155, intent to file
- 38 CFR 3.655, failure to report for a VA examination
- 38 USC 1110 and 1131, basic service connection
- 38 USC 1154(b), the combat rule for combat veterans' lay evidence
- M21-1, Part V, Subpart iii, Chapter 6, Digestive Disabilities
- VA.gov, Gulf War medically unexplained illnesses (functional GI presumptive)
- VA News, presumptive period extended through Dec. 31, 2026