VA TBI Claims Guide
Residuals of traumatic brain injury (TBI) are some of the most complex disabilities the VA rates, because a single head injury can affect thinking, mood, and the body all at once. This guide walks the whole path: how service connection works at a high level, how a TBI is service connected directly or through a presumptive or ordinary secondary pathway, what evidence wins, why these claims get denied, a checklist before you file, what the claims process looks like step by step, how to read your decision letter, and what to do whether you win or you're denied. You will also learn how TBI residuals are rated under diagnostic code 8045, including the 10-facet cognitive table and its highest-facet mapping rule.
What the VA Counts as Residuals of traumatic brain injury (TBI)
DC 8045 does not rate the brain injury itself. It rates the lasting effects, called residuals, that remain after a traumatic brain injury. Under 38 CFR 4.124a, the regulation states that "there are three main areas of dysfunction that may result from TBI and have profound effects on functioning: cognitive (which is common in varying degrees after TBI), emotional/behavioral, and physical. Each of these areas of dysfunction may require evaluation."
Cognitive impairment
Defined in the regulation as decreased memory, concentration, attention, and executive functions of the brain. Executive functions include goal setting, planning, organizing, problem solving, judgment, and decision making. Symptoms can fluctuate in severity from day to day.
Subjective symptoms
Symptoms you report that may be the only residual of TBI, such as headaches, dizziness, or sensitivity to light and sound. These are scored under their own facet unless they have a distinct diagnosis (like migraine) that is rated under its own code.
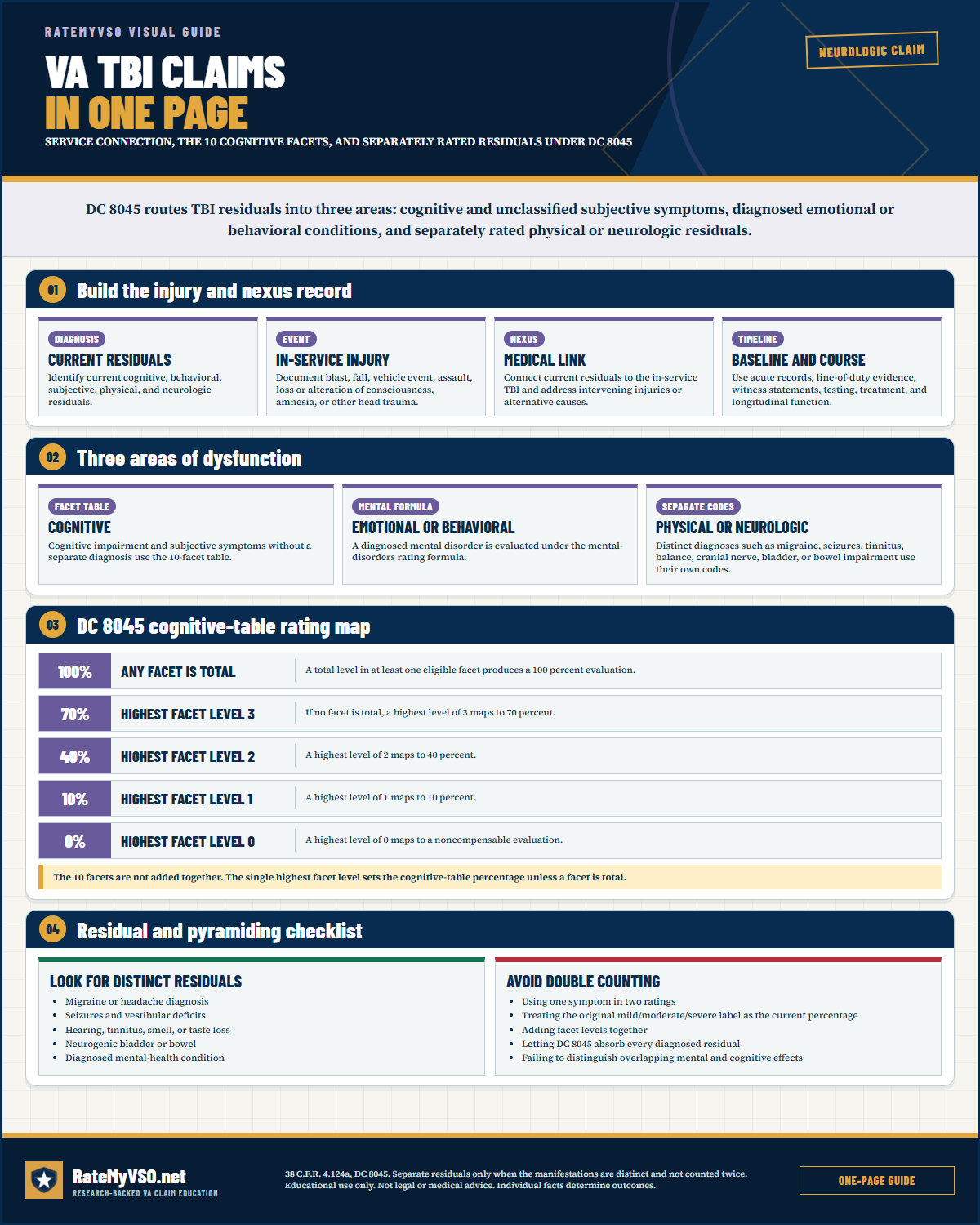 One-page guide: VA TBI Claims In One Page
See the injury file, three dysfunction areas, cognitive-facet conversion, and separate-residual rules. Opens the full-size chart, free to save or print.
One-page guide: VA TBI Claims In One Page
See the injury file, three dysfunction areas, cognitive-facet conversion, and separate-residual rules. Opens the full-size chart, free to save or print.
Symptoms Recorded in Granted Traumatic brain injury Decisions
We analyzed 1,385 granted Board decisions involving traumatic brain injury for symptoms named in sentences about the condition (rating-criteria recitations excluded). Descriptive of the published record, what the Board wrote down, not a checklist of what to report.
Detected by phrase-reading the decision text with condition-specific vocabularies. Source: Board of Veterans' Appeals decisions, RateMyVSO analysis.
ICD-10 Diagnosis Codes
The ICD-10 diagnosis codes most commonly used for DC 8045, Residuals of traumatic brain injury (TBI) (the kind on your medical records, decision letter, or C&P exam report). VA rates the disability and its residuals, not the diagnosis itself, so coding can vary.
How Service Connection Works, At a High Level
Before getting into the specific pathways below, it helps to understand the three things every TBI claim ultimately has to show. This is the same basic test that applies to any VA disability claim (38 CFR § 3.303), just applied to this condition.
- A current diagnosis. A real, current diagnosis of a TBI, or of its lasting residuals, from a qualified doctor. This is the first hurdle, and it is where a large share of TBI claims are lost. Without a current diagnosis in the file, a case does not reach the other two elements, and a veteran's own report of symptoms, on its own, is not treated as equivalent to a diagnosis.
- An in-service event. Something that happened during service that could plausibly cause a brain injury, for example a blast, a fall, a motor vehicle accident, or combat exposure.
- A medical nexus. A doctor's opinion connecting the current TBI to that in-service event, and explaining the reasoning, not just stating a conclusion.
How Residuals of traumatic brain injury (TBI) Gets Service Connected
Service connection for TBI residuals runs through one of the pathways below: a direct claim, a pre-existing TBI made worse by service, a presumptive downstream condition, or ordinary secondary service connection for a downstream condition outside the presumptive windows.
Direct Service Connection
Direct service connection is the primary route for TBI. It requires an in-service head-injury event (a blast, a motor vehicle accident, a fall, or combat exposure), a current diagnosis of TBI residuals, and a medical nexus linking the two. This is why the two largest denial reasons in published Board decisions for DC 8045 are a missing nexus and a missing current diagnosis. The "no current diagnosis" denial is unusually high here, because claimed residuals are often not objectively shown on testing.
Aggravation of a Pre-Existing TBI
When a veteran had a documented head injury or diagnosed TBI predating military service that was worsened beyond its natural progression by that service, aggravation-based service connection under 38 CFR § 3.306 is available.
Presumptive secondaries after a service-connected TBI (38 CFR 3.310(d))
There is no toxic-exposure or PACT Act presumptive for TBI itself. A TBI is established by direct or in-service-injury service connection. The presumptive logic instead runs downstream. Under 38 CFR 3.310(d), once a TBI is service connected, five diagnosable illnesses are held to be the proximate result of that TBI, in the absence of clear evidence to the contrary, depending on the TBI severity classified at the time of injury and the time between injury and onset:
- Parkinsonism, including Parkinson's disease, following moderate or severe TBI.
- Unprovoked seizures following moderate or severe TBI.
- Dementias (specifically presenile dementia of the Alzheimer type, frontotemporal dementia, and dementia with Lewy bodies) if manifest within 15 years following moderate or severe TBI.
- Depression if manifest within 3 years of moderate or severe TBI, or within 12 months of mild TBI.
- Diseases of hormone deficiency that result from hypothalamo-pituitary changes if manifest within 12 months of moderate or severe TBI.
"Mild," "moderate," and "severe" here refer to the TBI severity classified at or near the time of injury, consistent with Note (4) above. See the presumptive check tool.
Ordinary secondary service connection (38 CFR 3.310(a) and (b))
Veterans who fall outside the severity or time windows of 3.310(d) can still pursue ordinary secondary service connection under 38 CFR 3.310 with a medical nexus. This pathway is heavily used and frequently successful for TBI residuals. Aggravation under 3.310(b) is also available where a non-service-connected condition is made worse by the TBI.
The secondary conditions section below summarizes what we found in the Board's published decisions for the most-claimed downstream pathways.
Secondary to TBI: headaches and migraine
Headaches are one of the most common physical TBI residuals. When a headache disorder has a distinct diagnosis such as migraine, it is rated under its own code (DC 8100) rather than the facet table. In published BVA decisions, migraine claimed secondary to TBI was granted in approximately 58% of those appeals (n = 57, published BVA decisions). See the migraine claims guide.
Secondary to TBI: a diagnosed mental disorder
When a mental disorder such as a depressive disorder is diagnosed alongside TBI, the emotional/behavioral effects are rated under the 4.130 mental-disorder formula. In published BVA decisions, an unspecified depressive disorder (DC 9435) claimed secondary to TBI was granted in approximately 49% of those appeals (n = 45, published BVA decisions). A related dataset shows depression secondary to TBI granted at a notably higher rate in a separate slice. See the depression claims guide.
Secondary to TBI: sleep apnea and other conditions
Obstructive sleep apnea is a frequently claimed TBI secondary. In published BVA decisions, sleep apnea (DC 6847) claimed secondary to TBI was granted in approximately 53% of those appeals (n = 149, published BVA decisions). Tinnitus (DC 6260) and Meniere's syndrome (DC 6205) are also commonly claimed alongside TBI. See the sleep apnea claims guide and nexus letters.
What VA Looks For: Tests, Records, and Diagnostic Codes
Whether you are filing for the TBI itself or a downstream secondary condition, the record VA actually reviews centers on a small set of documents and data points.
- Neuroimaging: CT and/or MRI of the brain, which documents structural injury and severity and supports dementia or parkinsonism workups.
- Neuropsychological (neurocognitive) testing: the objective testing evidence of memory, attention, concentration, and executive-function impairment that separates a level 1 subjective complaint from a level 2 or level 3 finding on the facet table.
- Service treatment records: documentation of the in-service blast, fall, motor vehicle accident, or combat exposure that caused the injury.
- The diagnostic codes involved: DC 8045 for the TBI residuals themselves, plus whatever code applies to a separately ratable residual or downstream condition, for example DC 8100 (migraine), DC 6260 (tinnitus), DC 9304 (dementia), DC 9411 (PTSD) or DC 9435 (depression), or an endocrine code for hormone-deficiency disease.
- The actual form the examiner fills out: a Disability Benefits Questionnaire (DBQ) specific to TBI, discussed in more detail later in this guide.
Evidence That Wins These Claims
We analyzed the Board's published decisions and found a private medical opinion is the highest-yield evidence for these claims:
- A current diagnosis, first. A qualified doctor's diagnosis of a current TBI or its residuals belongs in the file before anything else, since the claim cannot get past the first element without one.
- A nexus opinion that explains its reasoning. An opinion that connects a current TBI to the in-service event and explains why, ideally reviewing the veteran's records and the relevant medical literature, carries far more weight than a bare conclusion.
- Documentation of the in-service event: service records showing a blast exposure, a fall, a motor vehicle accident, or combat exposure support the in-service element directly.
- Buddy and lay statements: lay statements describing the in-service head injury and the changes family, a spouse, or people who served alongside the veteran observed over time can support the timeline and the in-service event. Competent lay evidence describing what was directly witnessed can carry real weight on its own for some points.
- Service treatment records: records documenting the in-service head injury (a blast, an accident, a fall) support the in-service event.
- An opinion from the right kind of specialist: the Board weighs a provider's expertise, and an opinion from a provider whose specialty actually covers brain injury, such as a physiatrist, neurologist, neurosurgeon, or psychiatrist, carries more weight than one from a provider opining outside their field.
Evidence Cited in Published Traumatic brain injury Decisions
We analyzed 21,733 published Board decisions involving traumatic brain injury for condition-specific evidence, counting only case-specific mentions (boilerplate recitations excluded). "Favorable" is the share of decisions citing that evidence where every issue was granted or the outcome was mixed; the baseline across all these decisions is 58.5%. Evidence appearing in a decision does not mean it decided the case. Descriptive of the published record, not a prediction.
Detected by phrase-reading the decision text with condition-specific vocabularies. Source: Board of Veterans' Appeals decisions, RateMyVSO analysis.
Board Grants, Dissected
The Board decisions reviewed here show that direct service connection for TBI residuals is granted when the record contains a documented in-service head injury (even if informally recorded), credible lay testimony connecting current symptoms to that injury, and a medical opinion that ties the current diagnosis to service. Board decisions are not binding precedent on future cases, but they show what kind of evidence has persuaded the Board in the past.
Buddy statement and private opinion overcome missing STR diagnosis Citation A26038689 (April 24, 2026), Hearing docket
The record: The veteran testified that he was subjected to multiple simulated grenade explosions near his head during a training exercise, resulting in a forehead laceration and later headaches. His service treatment records documented the laceration but not a TBI diagnosis. A fellow servicemember submitted a signed 2013 affidavit corroborating the incident and the veteran's headaches afterward. After the Board hearing, the veteran submitted a private physician's opinion, based on review of his military and VA records, finding it at least as likely as not that the training incident caused a TBI and that his chronic headaches were a residual of it. Two negative VA opinions were also in the file.
Why it won: The Board found the veteran's testimony credible because it was consistent over time and matched the documented laceration. It gave the buddy statement substantial weight and found the negative VA opinions of minimal value because they relied only on the absence of contemporaneous records and did not address the veteran's credible lay reports. With the private opinion and lay evidence in at least approximate balance with the negative evidence, the Board applied the benefit of the doubt.
Documented in-service fall plus private nexus opinion Citation A26037018 (April 21, 2026), Hearing docket
The record: Service treatment records documented that the veteran hit his head on a weightlifting bar in February 1995, lost consciousness for 5 to 10 minutes, and was diagnosed with a concussion. He struck his head again in April 1996. A VA treatment record from 2016 documented the veteran's report of ongoing memory loss and headaches. A private physician, Dr. R.P., reviewed the veteran's service and post-service records along with medical literature and opined it was at least as likely as not that the in-service head injury caused the veteran's current post-concussive syndrome.
Why it won: The Board found the private opinion highly probative because it was based on a review of the full record and explained its reasoning. No VA opinion contradicted it. The Board also noted the rule against seeking a new medical opinion when favorable evidence already in the file is unrefuted.
VA psychologist's post-deployment TBI screening supports chronic disease theory Citation A26036696 (April 21, 2026), Direct Review docket
The record: A VA psychologist diagnosed the veteran with TBI in a June 2013 record, less than a year after he left service. In that same record the veteran described being thrown from a vehicle and losing consciousness for four to five minutes during deployment. The veteran failed to appear for a later scheduled VA examination.
Why it won: The Board found the veteran's report of the in-service incident credible. Because TBI is an organic disease of the nervous system, it is on the list of chronic conditions that can be connected to service through chronicity and continuity of symptoms rather than a same-day diagnosis. Since the TBI was identified less than a year after separation and tied to an in-service event, the Board found it at least as likely as not related to service.
Undocumented head injuries established through credible testimony Citation A26035267 (April 15, 2026), Direct Review docket
The record: The veteran testified that he sustained repeated head injuries from hatches, doors, or falling objects while serving on a submarine, sometimes resulting in unconsciousness or bleeding, none of which was documented in his service treatment records. VA examiners in 2021 and 2023 diagnosed a current TBI. A private physician, Dr. J.M., reviewed the record and opined the TBI was at least as likely as not related to service, reasoning that the reported injuries were common among sailors. A November 2021 VA examiner had opined against a link, relying on the absence of documentation and the veteran's own silence about head injury on medical history forms in 1989 and 1993.
Why it won: The Board found the veteran's lay statements about the undocumented injuries competent, credible, and consistent with his known duties. It weighed the private opinion against the VA opinion and found the evidence in approximate balance, resolving doubt in the veteran's favor.
Why These Claims Get Denied
Beyond the general "no nexus" and "no diagnosis" reasons covered above, a few specific denial patterns show up often enough to call out on their own.
- No current diagnosis of TBI or its residuals. This is the single most common reason these claims fall short. A veteran can have a documented head-injury history and ongoing symptoms, but if no qualified doctor has actually diagnosed a current TBI or its residuals, the claim does not reach the in-service-event or nexus questions.
- Symptoms alone standing in for a diagnosis. Headaches, memory trouble, or irritability, on their own, are not treated as equivalent to a diagnosed TBI. The diagnosis has to be in the record.
- A bare opinion with no explanation. A diagnosis or nexus opinion that does not explain how the listed symptoms support a TBI, or that comes from a provider practicing outside the relevant specialty, is given little to no probative value.
- Other, more likely explanations left unaddressed. The Board looks at alternative causes. Where examiners agree that brain-imaging findings are at least as consistent with a congenital condition or another lifestyle factor as with an in-service injury, or where a clearly documented post-service injury better explains a current TBI, a claim that does not address those alternatives struggles.
- An unresolved willful-misconduct finding. If the record shows the underlying incident was not in the line of duty, for example because of impaired driving, that finding has to be confronted directly rather than left unanswered.
- Missed deadlines and missed exams. A late Board appeal without good cause, or a missed VA exam without rescheduling, can end a claim on procedural grounds alone, regardless of the medical merits.
The Three Areas of Dysfunction and How They Are Rated
The single most important thing to understand about DC 8045 is that the three areas of dysfunction are not all rated the same way. The regulation routes each one to a different place.
1. Cognitive dysfunction (the 10-facet table)
Cognitive impairment, plus any subjective symptoms that do not have their own diagnosis, are evaluated under the table titled "Evaluation of Cognitive Impairment and Other Residuals of TBI Not Otherwise Classified." This is the table that produces the 0, 10, 40, 70, or 100 percent rating. The 10 facets and the mapping rule are covered in the rating section below.
2. Emotional/behavioral dysfunction (rated under 4.130)
The regulation states: "Evaluate emotional/behavioral dysfunction under 4.130 (Schedule of ratings, mental disorders) when there is a diagnosis of a mental disorder." That means if you have a diagnosed mental health condition along with your TBI, the emotional and behavioral effects are rated under the 38 CFR 4.130 general rating formula for mental disorders, the same 0/10/30/50/70/100 formula used for depression and PTSD. When there is no diagnosed mental disorder, the emotional/behavioral symptoms are scored under the neurobehavioral effects facet in the cognitive table instead.
3. Physical (including neurological) dysfunction (rated under its own codes)
Physical residuals are not folded into the facet table. The regulation lists examples to be rated under their own appropriate diagnostic code: "Motor and sensory dysfunction, including pain, of the extremities and face; visual impairment; hearing loss and tinnitus; loss of sense of smell and taste; seizures; gait, coordination, and balance problems; speech and other communication difficulties... neurogenic bladder; neurogenic bowel; cranial nerve dysfunctions; autonomic nerve dysfunctions; and endocrine dysfunctions." Common examples include migraine headaches (DC 8100), tinnitus (DC 6260), and sleep problems. Each is rated separately and then combined under 38 CFR 4.25.
DC 8045 Rating Levels
The overall percentage for the cognitive table is set by a single rule, quoted verbatim from 38 CFR 4.124a: "Assign a 100-percent evaluation if 'total' is the level of evaluation for one or more facets. If no facet is evaluated as 'total,' assign the overall percentage evaluation based on the level of the highest facet as follows: 0 = 0 percent; 1 = 10 percent; 2 = 40 percent; and 3 = 70 percent."
In plain language: the VA scores each of the 10 facets from 0 to 3 (or "total"), then looks only at your single highest facet level and converts that one number into your rating. Adding up multiple facets does not raise the rating. One facet at level 3 produces the same 70 percent as five facets at level 3.
Go deeper: open the full TBI residuals breakdown- What the VA measures at your C&P exam
- Evidence that has won at the Board
- Inside the rater's playbook: grant, denial, and remand rates
- Secondary condition map
The 10 facets of the cognitive impairment table
The table below catalogues the 10 facets and what each scored level means, summarized from the verbatim regulation. Note that not every facet has every level: Social interaction, Subjective symptoms, and Neurobehavioral effects have no "total" level. Subjective symptoms has no level 3. Consciousness has only a "total" level.
| Facet | What the levels measure (0 lowest to 3 / total highest) |
|---|---|
| Memory, attention, concentration, executive functions | 0: no complaints. 1: a complaint of mild loss but without objective evidence on testing. 2: objective testing evidence of mild impairment with mild functional impairment. 3: objective testing evidence of moderate impairment with moderate functional impairment. Total: objective testing evidence of severe impairment with severe functional impairment. |
| Judgment | 0: normal. 1: mildly impaired (occasionally unable to weigh alternatives for complex or unfamiliar decisions). 2: moderately impaired (usually unable for complex decisions, little difficulty with simple ones). 3: moderately severely impaired (occasionally unable even for routine decisions). Total: severely impaired (usually unable even for routine decisions, for example cannot judge appropriate clothing for the weather). |
| Social interaction | 0: routinely appropriate. 1: occasionally inappropriate. 2: frequently inappropriate. 3: inappropriate most or all of the time. (No "total" level.) |
| Orientation | 0: always oriented to person, time, place, situation. 1: occasionally disoriented to one of the four aspects. 2: occasionally disoriented to two aspects, or often to one. 3: often disoriented to two or more aspects. Total: consistently disoriented to two or more aspects. |
| Motor activity (with intact motor and sensory system) | 0: normal. 1: normal most of the time but mildly slowed at times due to apraxia. 2: mildly decreased or with moderate slowing due to apraxia. 3: moderately decreased due to apraxia. Total: severely decreased due to apraxia. |
| Visual spatial orientation | 0: normal. 1: mildly impaired (occasionally gets lost in unfamiliar surroundings, can use GPS). 2: moderately impaired (usually gets lost in unfamiliar surroundings, difficulty using GPS). 3: moderately severely impaired (gets lost even in familiar surroundings, cannot use GPS). Total: severely impaired (may be unable to name own body parts or find the way between rooms in a familiar place). |
| Subjective symptoms | 0: symptoms that do not interfere with work, daily living, or relationships (for example mild or occasional headaches, mild anxiety). 1: three or more symptoms that mildly interfere (for example intermittent dizziness, daily mild to moderate headaches, tinnitus, frequent insomnia, sensitivity to sound or light). 2: three or more symptoms that moderately interfere (for example marked fatigability, blurred or double vision, headaches requiring rest periods most days). (No level 3 or "total.") |
| Neurobehavioral effects | 0: one or more effects (such as irritability, impulsivity, lack of motivation, verbal or physical aggression, apathy, moodiness) that do not interfere with workplace or social interaction. 1: effects that occasionally interfere but do not preclude interaction. 2: effects that frequently interfere but do not preclude interaction. 3: effects that interfere with or preclude interaction on most days, or occasionally require supervision for safety. (No "total" level.) |
| Communication | 0: able to communicate and comprehend spoken and written language. 1: comprehension or expression only occasionally impaired, can communicate complex ideas. 2: unable to communicate or comprehend more than occasionally but less than half the time, generally communicates complex ideas. 3: unable at least half the time but not all the time, can communicate basic needs. Total: complete inability to communicate or comprehend, unable to communicate basic needs. |
| Consciousness | Total only: persistently altered state of consciousness, such as a vegetative state, minimally responsive state, or coma. (This facet has no other level. Any altered consciousness is totally disabling.) |
Special monthly compensation (SMC): DC 8045 directs the rater to "consider the need for special monthly compensation for such problems as loss of use of an extremity, certain sensory impairments, erectile dysfunction, the need for aid and attendance (including for protection from hazards or dangers incident to the daily environment due to cognitive impairment), being housebound, etc." SMC is an extra payment on top of the schedular rating. The FAQ below covers how SMC commonly applies in TBI claims.
Notes from the regulation:
- Note (1): When a TBI residual overlaps with a comorbid mental, neurologic, or other physical disorder, do not assign more than one evaluation based on the same manifestations. If the symptoms cannot be clearly separated, assign a single evaluation under whichever criteria better assess the overall impairment. If they are clearly separable, rate each separately.
- Note (2): The symptoms listed as examples at certain levels are only examples, not symptoms that must all be present to assign a level.
- Note (3): "Instrumental activities of daily living" means activities other than self-care that are needed for independent living (meal preparation, housework, shopping, traveling, laundry, managing one's own medications, using a telephone), distinct from basic "activities of daily living" like bathing, dressing, and eating.
- Note (4): The terms "mild," "moderate," and "severe" TBI in medical records refer to a classification made at or near the time of injury, not to the current level of functioning. This classification does not affect the rating assigned under DC 8045.
- Note (5): A veteran whose TBI residuals were rated under a version of DC 8045 in effect before October 23, 2008 may request review under the current criteria, regardless of whether the disability has worsened. The request is treated as a claim for an increased rating, but the award cannot be effective before October 23, 2008.
Pyramiding and Rating Separately
The VA's pyramiding rule at 38 CFR 4.14 prevents paying twice for the same symptoms. For TBI, the regulation builds this in two ways.
First, DC 8045 directs that physical residuals with a distinct diagnosis (migraine, Meniere's disease, seizures, hearing loss and tinnitus, neurogenic bladder, neurogenic bowel, and similar) are evaluated under their own diagnostic codes and combined under 38 CFR 4.25. A diagnosed mental disorder is rated under the 4.130 formula. So a complete TBI picture is often more than just the "8045" rating. The separately diagnosed residuals carry their own percentages, and the cognitive-table evaluation counts as a single condition for combining purposes. In practice this means a veteran can be rated separately for a TBI and for a distinct condition like a headache disorder or a mood disorder that arose alongside it, as long as the symptoms driving each rating do not overlap.
Second, Note (1) to DC 8045 bars double-counting. Where a TBI residual in the facet table overlaps with a comorbid mental or neurologic diagnosis, the same manifestations cannot support more than one evaluation. If the symptoms cannot be clearly separated, the rater assigns one evaluation under whichever criteria better capture the overall impairment. If they are clearly separable, each is rated separately. In practice this means the headache symptom that is being rated as migraine under DC 8100 should not also be the symptom driving the Subjective symptoms facet in the cognitive table.
Common Mistakes
Published Board decisions and the VA's adjudication manual (M21-1, Part V, Subpart iii, Chapter 12, Section B) surface the same recurring errors:
- Confusing the at-injury severity label with the current rating: records calling a TBI "mild," "moderate," or "severe" describe the injury near the time it happened, not present functioning. Per Note (4), that label does not set the rating, which is driven entirely by the current 10-facet evaluation.
- Letting one global TBI percentage absorb separately ratable residuals: distinct-diagnosis conditions like migraine, Meniere's disease, seizures, hearing loss and tinnitus, neurogenic bladder or bowel, and a diagnosed mental disorder (rated under 4.130) are meant to be evaluated under their own codes and combined under 4.25. Claiming only "8045" can understate the overall picture.
- Filing for a TBI-secondary condition with no medical nexus: "no nexus" is the single largest denial reason for DC 8045, and the published data show a private nexus opinion is associated with a much higher grant rate.
- Claiming a 3.310(d) presumptive without meeting the thresholds: parkinsonism, dementia, depression, seizures, and hormone deficiency are presumptive only within set severity-and-time windows. Outside those windows, ordinary secondary service connection under 3.310(a) is still available with a nexus.
- Reporting only subjective complaints without neuropsychological testing: an unconfirmed complaint tends to score a facet at level 1 (10 percent), while objective testing evidence is what supports level 2 (40 percent) or level 3 (70 percent).
- Double-counting the same symptoms: using the identical manifestation across the facet table and a comorbid mental or neurologic diagnosis is barred by Note (1) and 38 CFR 4.14.
- Not knowing about the pre-October 23, 2008 review right: under Note (5), veterans rated under the older 8045 criteria can request re-evaluation under the current criteria regardless of whether the condition has worsened.
Do's and Don'ts
A condensed version of everything above, in the order it actually matters when you sit down to build your file.
- Get a current diagnosis of TBI or its residuals from a qualified doctor before anything else.
- Get a nexus opinion that explains its reasoning, not just its conclusion, ideally reviewing your records and the relevant medical literature.
- Document the specific in-service event, a blast, a fall, a vehicle accident, or combat exposure, with service records where available.
- Use lay and buddy statements describing what happened and the changes others observed over time.
- Make sure any nexus opinion comes from a provider whose specialty actually covers brain injury (a physiatrist, neurologist, neurosurgeon, or psychiatrist), not a provider outside that field.
- If the evidence is genuinely close, ask that reasonable doubt be resolved in your favor.
- Address any post-service head injuries, alternative causes, or misconduct findings directly rather than leaving them unanswered.
- Attend every scheduled VA exam, and reschedule immediately if you cannot make it.
- File a Board appeal within one year of your decision letter, and calendar the deadline.
- Don't assume a documented head-injury history or symptoms alone will prove a current TBI, get the diagnosis in the record.
- Don't submit a bare conclusion with no reasoning behind it as your nexus evidence.
- Don't ignore other plausible explanations for your brain-imaging findings, such as a congenital condition, another documented cause, or a later post-service injury.
- Don't let a willful-misconduct finding go unanswered.
- Don't miss the one-year window to appeal to the Board, being unsure of the deadline is not treated as good cause for a late filing.
- Don't skip a scheduled VA exam without rescheduling, missing one without good cause can result in denial as a matter of law.
- Don't assume one global TBI percentage covers everything, distinctly diagnosed residuals like migraine or a mental-health condition are meant to be rated separately and combined.
Quick Checklist Before You File
Bring these together before you submit anything.
- A current diagnosis of TBI or its residuals from a qualified doctor.
- Documentation of the in-service event (a blast, fall, vehicle accident, or combat exposure), including service records.
- A nexus opinion that reviews your records and explains the reasoning behind its conclusion.
- Lay and buddy statements describing the event and your ongoing symptoms.
- Confirmation that any nexus opinion comes from a provider whose specialty covers brain injury.
- Documentation addressing any post-service head injuries, other possible causes, or misconduct findings.
- Your calendar marked for every scheduled VA exam and the one-year Board appeal deadline.
For the mechanics of actually submitting the claim, see the Standard Claim Guide and the Fully Developed Claim Guide (filing with all your evidence up front can speed up the decision).
The Claims Process, Step by Step
Once you file, your claim moves through a series of hand-offs. Understanding who does what helps you know who to contact, and what to expect, at each stage.
- You file the claim. Directly with VA, through VA.gov, or with the help of an accredited representative.
- VA acknowledges the claim and assigns it for development. A Veteran Service Representative (VSR) is assigned to gather your service treatment records, VA and private medical records, and any other evidence needed.
- The VSR orders a Compensation & Pension (C&P) exam if one is needed. Most TBI claims require one, especially where a nexus opinion or a facet-by-facet cognitive evaluation is needed.
- The C&P exam is conducted. By a VA clinician or a contracted examiner, who completes a Disability Benefits Questionnaire (DBQ) documenting the diagnosis, severity across the 10 facets, and, where relevant, a nexus opinion.
- The file goes to a Rating Veteran Service Representative (RVSR), the "rater." The rater reviews the complete file, including the exam results, and decides whether service connection is warranted and at what percentage.
- A senior reviewer may review the decision before it's finalized, depending on the complexity of the claim.
- VA issues the decision letter. This states whether the claim is granted or denied, the rating percentage if granted, and the reasons behind the decision.
- If you disagree, you choose an appeal lane. Higher-Level Review, Supplemental Claim, or a Board appeal, covered later in this guide.
Who's who: VSO vs. VSR vs. Rater vs. C&P Examiner
Your VSO
An accredited representative from a veterans service organization, or an accredited attorney or claims agent. Not a VA employee. Helps you prepare, gather evidence, and file, and can represent you through an appeal. Has no authority to decide your claim.
VSR (Veteran Service Representative)
VA staff who "develops" your claim: requests records, schedules the C&P exam, and assembles the file. Does not decide the rating.
Rater (RVSR)
VA staff who reviews the completed file and makes the actual decision, service connection or denial, and the percentage. This is the person whose judgment the decision letter reflects.
C&P Examiner
A VA clinician or a contracted medical examiner who conducts the exam and completes the DBQ. Documents findings and, where asked, a nexus opinion. Does not decide the claim.
For the full walkthrough of every stage with more detail, see Inside Your Claim and Claim Stages.
DBQs and Your C&P Exam
The VA structures the TBI exam around the 10 facets of 38 CFR 4.124a. The tests and forms below are what the adjudication manual and exam templates rely on:
- The TBI DBQ (VA Form 21-0960c-1): the "Initial Evaluation of Residuals of Traumatic Brain Injury" or Review TBI Disability Benefits Questionnaire is built around the 10 facets. See the DBQ guide for how these forms work generally, including whether a private DBQ can be submitted instead of relying solely on a VA exam.
- A comprehensive TBI examination by a specialist: the VA requires the initial or comprehensive TBI exam to be performed by one of four specialties, a physiatrist, neurologist, neurosurgeon, or psychiatrist.
- Neuropsychological (neurocognitive) testing: provides the objective evidence of memory, attention, concentration, and executive-function impairment that supports facets at level 2 or 3 rather than a level 1 subjective complaint.
- Neuroimaging (CT and/or MRI of the brain): documents structural injury and severity and supports dementia or parkinsonism workups.
- A mental health DBQ or examination under 4.130: used when there is a separately diagnosed mental disorder (for example a depressive disorder or PTSD) arising with the TBI.
- Condition-specific DBQs and tests for separately ratable physical residuals: the headache or migraine DBQ, the seizure (epilepsy) DBQ and EEG, an audiology exam for hearing loss and tinnitus, an eye and visual exam, a smell and taste evaluation, endocrine and hormone panels for hypothalamic-pituitary deficiency, and a gait, balance, and coordination assessment.
Before your C&P exam, bring a clear, specific account of your symptoms across all three areas of dysfunction, cognitive, emotional/behavioral, and physical, and focus on how the condition affects daily function, not just how you feel on an average day. Be consistent with what's already in your medical records and prior statements. For a full walkthrough of what to expect and how to prepare, see the C&P Exam Prep Guide.
Reading Your Decision Letter, and What to Do If Denied
Your decision letter has two parts: a narrative section explaining the reasoning (often called "reasons and bases"), and a codesheet showing the actual rating percentage, the effective date, and the diagnostic code used. See the Reading Your Decision Letter Guide for how to find and interpret each part, or use the Letter Interpreter tool to upload your own letter and get a plain-English breakdown.
If your claim is denied, or the rating is lower than you expected, you have three main lanes:
- Supplemental Claim: refile with new and relevant evidence, such as a new nexus opinion or updated neuropsychological testing. See Supplemental Claim Guide.
- Higher-Level Review (HLR): a senior reviewer looks at the same evidence again for a difference of opinion, no new evidence is added. See HLR Guide.
- Board Appeal: your case goes to a Veterans Law Judge at the Board of Veterans' Appeals, with options for a direct review, an evidence docket, or a hearing. See Board Appeal Guide. You generally have one year from your decision letter to file, and being unsure of the deadline is not treated as good cause for filing late.
Not sure which lane fits your situation? See the Appeals decision guide for a side-by-side comparison of all three.
After You Win: Maintaining Your Rating
A grant is not always the end of the story. Keep your treatment consistent, continued follow-up with a neurologist or the relevant specialist, and records documenting your facet-level symptoms over time, protects you if VA schedules a future reexamination. Not every rating gets reexamined; understand when a rating becomes protected from future review (including Permanent and Total status) and what to do if VA proposes to reduce it. See Protect Your Rating and Future Reexaminations for the specifics.
If your TBI residuals worsen after the initial grant, for example a facet moving up a level, you can file for an increased rating. See the Rating Increase Guide.
Your effective date is generally the date VA received your claim or your intent to file, not the date the injury happened, so filing promptly matters even while you're still gathering evidence. See Standard Claim Guide for how an intent to file can protect an earlier effective date.
Common Secondary Conditions
TBI sits at the center of a web of related claims that runs in both directions. Some conditions are claimed as caused or aggravated by a service-connected TBI. Others are conditions that veterans claim a TBI was caused by or occurred alongside. The published Board data below shows grant rates for each direction. All figures are grant rates (appeals granted divided by decisions) paired with the sample size.
Conditions that can lead to a TBI (TBI as the secondary)
Claims where a TBI itself was argued as secondary to an already service-connected condition. This is a less common direction than the ones below, since a TBI is usually established directly through an in-service head injury, but where the published data supports it, this is the "ways to connect via another condition" list for a TBI claim:
Conditions a service-connected TBI commonly causes or aggravates
These are conditions claimed as secondary to (downstream of) a TBI. We found each bar is the published BVA grant rate, with the number of decisions below it:
Conditions commonly claimed alongside or before a TBI claim
These are conditions where a TBI was argued to be connected to, or to co-occur with, another claimed condition. Treat these as co-occurring patterns rather than strict causation. We found each bar is the published BVA grant rate:
Quick Reference Tables
TBI Service Connection Pathways
| Pathway | Requirement | Evidence Needed |
|---|---|---|
| Direct service connection | In-service blast, fall, motor vehicle accident, or combat exposure | Current diagnosis + service records + nexus opinion linking the two |
| Aggravation of a pre-existing TBI | Documented pre-service head injury worsened beyond natural progression by service | Pre-service baseline + records showing worsening during or after service |
| Presumptive downstream condition (38 CFR 3.310(d)) | Parkinsonism, seizures, dementia, depression, or hormone deficiency within the set severity-and-time window | Service-connected TBI + diagnosis of the downstream condition within the window |
| Ordinary secondary (38 CFR 3.310(a)/(b)) | A downstream condition outside the 3.310(d) windows, caused or aggravated by the TBI | Service-connected TBI + medical nexus addressing causation or aggravation |
3.310(d) Presumptive Secondary Conditions
| Condition | TBI Severity Required | Time Window |
|---|---|---|
| Parkinsonism (incl. Parkinson's disease) | Moderate or severe | No stated limit |
| Unprovoked seizures | Moderate or severe | No stated limit |
| Dementias (Alzheimer type, frontotemporal, Lewy body) | Moderate or severe | Within 15 years of the TBI |
| Depression | Moderate or severe, or mild | Within 3 years (moderate/severe) or 12 months (mild) |
| Hormone-deficiency disease (hypothalamo-pituitary) | Moderate or severe | Within 12 months of the TBI |
From Filing to Decision: Who Does What
| Role | Does | Decides your rating? |
|---|---|---|
| VSO / accredited representative | Helps prepare, gather evidence, and file; represents you on appeal | No |
| VSR | Develops the claim: orders records and the C&P exam | No |
| C&P Examiner | Conducts the exam, completes the DBQ, may give a nexus opinion | No / but has a strong impact |
| Rater (RVSR) | Reviews the full file and decides service connection and percentage | Yes |
Frequently Asked Questions
How does the VA turn the 10-facet table into a single percentage?
My records say my TBI was "mild." Does that limit my rating?
Can I be rated separately for my TBI and for my headaches or depression?
What conditions are presumed to be caused by a service-connected TBI?
Is there a PACT Act or Agent Orange presumptive for TBI itself?
Can a TBI lead to special monthly compensation (SMC)?
What if my head injury happened during Reserve or National Guard training?
Does an injury from my own misconduct count?
Related Tools and Guides
Sources
- 38 CFR 4.124a, DC 8045, residuals of traumatic brain injury, rating by facets
- 38 CFR 3.303, basic rules for service connection (current disability, in-service event, and nexus)
- 38 CFR 3.310, secondary service connection, including 3.310(d) TBI presumptive secondaries
- 38 CFR 3.306, aggravation of pre-existing disability
- 38 CFR 3.301, willful misconduct and line of duty
- 38 CFR 3.6, active duty, ACDUTRA, and INACDUTRA
- 38 CFR 3.655, denial for failing to report for a VA examination
- 38 CFR 3.400, effective dates
- 38 CFR 3.102, benefit of the doubt when evidence is in balance
- 38 CFR 20.203, timeliness of a Board appeal and extensions
- 38 CFR 4.14, no pyramiding of overlapping symptoms
- 38 USC 1110 and 38 USC 5107(b), basic entitlement and benefit of the doubt
- Shedden v. Principi, 381 F.3d 1163 (Fed. Cir. 2004); Hickson v. West, 12 Vet. App. 247 (1999), the three-element test for service connection
- Nieves-Rodriguez v. Peake, 22 Vet. App. 295 (2008), a medical opinion's probative value comes from its reasoning
- McClain v. Nicholson, 21 Vet. App. 319 (2007); Romanowsky v. Shinseki, 26 Vet. App. 289 (2013), current disability at or near the time of filing
- Lynch v. McDonough, 21 F.4th 776 (Fed. Cir. 2021), benefit of the doubt applies only when the evidence is nearly equal
- VA.gov, VA to expand benefits for traumatic brain injury (3.310(d) presumptive secondaries)
- VA.gov, traumatic brain injury research overview
- M21-1, Part V, Subpart iii, Chapter 12, Section B, Traumatic Brain Injury
This guide is educational, not legal or medical advice, and not a prediction of any individual claim outcome. Rating criteria can change. Confirm current details in 38 CFR 4.124a. For help with your own claim, talk to a VA-accredited representative.