VA Coronary Artery Disease Claims Guide
Coronary artery disease (CAD) is what the VA calls ischemic heart disease, and that single fact shapes most of these claims. Ischemic heart disease is an Agent Orange presumptive condition, so a veteran with qualifying herbicide exposure can have CAD recognized as service connected without proving a medical nexus. CAD is rated under diagnostic code 7005 using a General Rating Formula for the heart that runs on METs (a measure of physical workload), not on ejection fraction. This guide explains how service connection works at a high level, the presumptive path, the current MET-based rating levels, the direct and secondary routes to service connection, the evidence we found wins these claims, why claims get denied, the claims process step by step, and what to do whether you win or you're denied.
What the VA Counts as Coronary Artery Disease (Ischemic Heart Disease)
Coronary artery disease, ischemic heart disease, and arteriosclerotic heart disease all describe the same underlying problem: the arteries that feed the heart muscle narrow and harden, so the heart does not get enough oxygen-rich blood. Left untreated, this narrowing can lead to a heart attack (myocardial infarction). The VA rates this condition under 38 CFR 4.104, diagnostic code 7005, titled "Arteriosclerotic heart disease (coronary artery disease)." The VA's public health materials state plainly that ischemic heart disease is "also known as coronary artery disease or hardening of the arteries." VA law treats this condition more favorably than many others, both because it sits on the Agent Orange presumptive list and because it is often linked to other conditions veterans already carry a service connection for.
What is included
The VA defines ischemic heart disease to include coronary artery disease and the residuals of a heart attack (myocardial infarction). A single DBQ, the Ischemic Heart Disease questionnaire, covers all of it. Coronary bypass surgery and stents fall under this same code.
What is NOT included
The VA's definition of ischemic heart disease specifically excludes hypertension (high blood pressure) and peripheral manifestations of arteriosclerosis, such as peripheral artery disease and stroke. Those are separate conditions rated under different diagnostic codes.
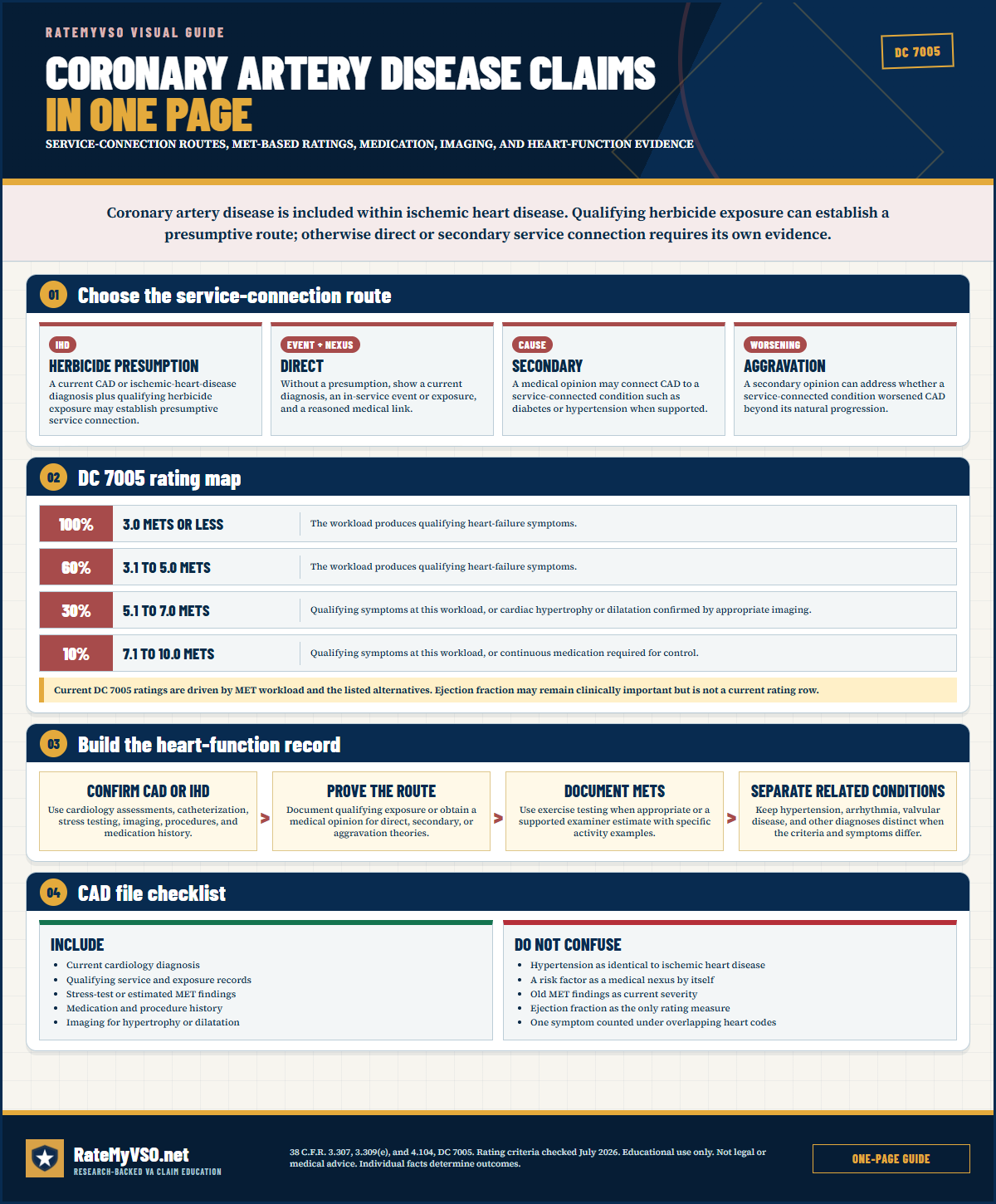 One-page guide: Coronary Artery Disease Claims In One Page
See presumptive, direct, secondary, and aggravation routes plus the current MET-based DC 7005 tiers. Opens the full-size chart, free to save or print.
One-page guide: Coronary Artery Disease Claims In One Page
See presumptive, direct, secondary, and aggravation routes plus the current MET-based DC 7005 tiers. Opens the full-size chart, free to save or print.
ICD-10 Diagnosis Codes
The ICD-10 diagnosis codes most commonly used for DC 7005, Arteriosclerotic heart disease (coronary artery disease) (the kind on your medical records, decision letter, or C&P exam report). VA rates the disability and its residuals, not the diagnosis itself, so coding can vary.
How Service Connection Works, At a High Level
Before getting into the specific pathways below, it helps to understand the three things every heart disease claim ultimately has to show on a direct basis. This is the same basic test that applies to any VA disability claim, just applied to this condition.
- A current diagnosis of heart disease. VA must see that you actually have coronary artery disease or ischemic heart disease now. A VA or private medical record showing the diagnosis is usually enough, and VA often concedes this element up front once a record is in the file.
- An in-service cause or event. You must tie the disease to something in service, such as herbicide (Agent Orange) exposure, another toxic exposure, or a service-connected condition behind it. Claims fail where no in-service cause is shown at all.
- A medical link (nexus). For claims that are not presumptive, you need a medical opinion connecting your heart disease to service. An opinion that explains its reasoning carries far more weight than one that simply states a conclusion.
How Coronary Artery Disease (Ischemic Heart Disease) Gets Service Connected
Established pathways to service connection for CAD, including the secondary theories the Board sees most:
Agent Orange presumptive (the dominant path)
Ischemic heart disease, which the VA defines to include coronary artery disease, is an Agent Orange / herbicide presumptive condition under 38 CFR 3.309(e). The official VA Public Health page describes ischemic heart disease as "also known as coronary artery disease" and states that veterans who develop it after qualifying herbicide exposure "do not have to prove a connection between their disease and service." Ischemic heart disease was added to the presumptive list in 2010.
When this presumption applies, two of the three usual elements (an in-service event and a medical nexus) are presumed. The veteran needs a current ischemic heart disease diagnosis and qualifying herbicide exposure, for example service in Vietnam between January 1962 and May 1975, on or near a U.S. or Royal Thai base in Thailand between 1962 and 1976 regardless of where on the base the veteran served, service near the Korea DMZ during the covered dates, Johnston Atoll, and other locations and dates catalogued in the VA's adjudication manual, M21-1. See the Agent Orange presumptive page. The PACT Act is what extended the herbicide presumption to those Thailand bases and added the separate Korea DMZ presumption. The reach of this presumption is the main reason the measured nexus benefit for CAD is comparatively small (see the evidence section below): for many exposed veterans, no nexus letter is needed at all.
Credible, consistent service statements can carry the exposure element. Even when official records of a veteran's exact location are incomplete, statements that are consistent with the veteran's known service and are backed by whatever service records do exist can establish qualifying exposure. Under the benefit-of-the-doubt rule, when the evidence for and against a veteran's account is about equal, VA must decide in the veteran's favor. This has helped veterans whose service near a base perimeter or the DMZ was credible but not fully documented in surviving records.
Direct service connection
When the presumption does not apply, direct service connection requires three elements: a current CAD diagnosis, an in-service event or risk exposure, and a medical nexus opinion linking the two. We analyzed the Board's published decisions and found the absence of that nexus is the single biggest reason direct CAD claims are denied, ahead of no current diagnosis and no qualifying in-service event.
Secondary to diabetes (38 CFR 3.310)
Diabetes damages blood vessels over time and is a leading cause of coronary artery disease. CAD claimed as secondary to service-connected diabetes is the highest-volume secondary pathway for this code in the Board's data. A secondary claim turns on a medical opinion connecting the service-connected diabetes to the heart disease, and a detailed opinion that walks through the reasoning and addresses other risk factors carries the most weight, particularly where it outweighs opinions filed against the claim. See the diabetes claims guide.
Secondary to hypertension (38 CFR 3.310)
Long-standing high blood pressure forces the heart to work harder and accelerates arterial disease, so CAD is also frequently claimed secondary to service-connected hypertension. Because hypertension itself is now separately presumptive under the PACT Act for Agent Orange veterans, this two-step path (presumptive hypertension, then CAD secondary to it) appears in published decisions, and heart disease caused by an already service-connected hypertension or diabetes can be granted even with no direct link to service in the file. See the hypertension claims guide.
Secondary to PTSD (DC 9411)
The Board has granted CAD secondary to service-connected PTSD, where a doctor explains how the prolonged stress response of PTSD (elevated stress hormones, higher blood pressure, chronic inflammation) contributes to heart disease over time. In the Board's published decisions this pathway appears in nearly as many appeals as the diabetes pathway above, and it often runs alongside the hypertension theory, since PTSD and hypertension frequently sit in the same file. The medical opinion that walks through the mechanism is what decides these claims. See the PTSD claims guide and the Board-data page for CAD secondary to PTSD.
Secondary to sleep apnea (38 CFR 3.310)
Obstructive sleep apnea strains the cardiovascular system through repeated drops in blood oxygen. CAD claimed secondary to service-connected sleep apnea is lower volume but has been a viable pathway in published decisions. A medical nexus opinion is the central document for any of these secondary theories. See the sleep apnea claims guide.
What VA Looks For: Tests, Records, and Diagnostic Codes
Whether you are filing on a presumptive, direct, or secondary basis, the record VA actually reviews centers on a small set of documents and data points.
- A current diagnosis in the file: a VA or private record that names coronary artery disease or ischemic heart disease. Every published grant in this area starts here.
- Proof of qualifying service, place, and dates: for the herbicide presumption, service records or a credible, consistent statement placing you in Vietnam, on or near a covered Thailand base, near the Korea DMZ, or another location and date range the presumption covers.
- The diagnostic codes involved: DC 7005 for the coronary artery disease itself, plus whatever code applies to a condition you're connecting it to, for example DC 7101 (hypertension) or the diabetes diagnostic codes if you're arguing a secondary theory.
- The actual form the examiner fills out: the Ischemic Heart Disease Disability Benefits Questionnaire (DBQ), covered in more detail later in this guide.
Evidence That Wins These Claims
We analyzed the Board's published decisions and found a private medical opinion is the highest-yield evidence for these claims. A private opinion that explicitly states the service link, and explains its reasoning rather than just asserting a conclusion, is what most distinguishes granted DC 7005 decisions from denied ones. See nexus letters.
The private-opinion benefit is real but comparatively modest for this code, and the reason is the presumption. The gap below is the smallest among the conditions in this guide series, which the data attributes to the Agent Orange ischemic heart disease presumption: many CAD grants run through the presumption and need no nexus at all.
Current diagnosis in the record: every published grant starts with a VA or private record naming the coronary artery disease or ischemic heart disease diagnosis, and VA frequently concedes this element once that record is in the file.
Proof of qualifying exposure: for presumptive claims, service records or a clear, consistent personal statement establishing service in a covered location and time window.
A medical opinion that addresses the mechanism: for secondary and non-presumptive direct claims, an opinion that explains how diabetes, hypertension, PTSD, or another condition contributed to the heart disease, rather than a bare statement that service "could have" caused it, is what typically outweighs opinions filed against the claim.
Evidence Cited in Published Coronary artery disease Decisions
We analyzed 30,447 published Board decisions involving coronary artery disease for condition-specific evidence, counting only case-specific mentions (boilerplate recitations excluded). "Favorable" is the share of decisions citing that evidence where every issue was granted or the outcome was mixed; the baseline across all these decisions is 54%, combining every diagnostic code below. Evidence appearing in a decision does not mean it decided the case. Descriptive of the published record, not a prediction.
By diagnostic code
These codes are grouped together above. They do not perform the same, so find your own code here rather than reading the combined figure. Codes retired in the schedule rewrites are left out, because their old decisions were judged under criteria that no longer apply.
Detected by phrase-reading the decision text with condition-specific vocabularies. Source: Board of Veterans' Appeals decisions, RateMyVSO analysis.
Board Grants, Dissected
The Board decisions below show that veterans have won direct or presumptive service connection for coronary artery disease (CAD) or ischemic heart disease (IHD) under several different theories: herbicide exposure at Thailand air bases or other posts, exposure tied to Gulf War service, and secondary connection through tobacco use caused by a service-connected mental health condition. Board decisions are not binding precedent, and each case turned on its own facts and evidence.
Facts-found herbicide exposure at Thailand air base wins CAD grant Citation A26038368 (April 23, 2026), Direct Review docket
The record: The Veteran served at U-Tapao and Nakhon Phanom Royal Thai Air Force Bases during the Vietnam era. Military personnel records confirmed these duty stations. In a sworn declaration, the Veteran stated his duties as a munitions specialist took him near the base perimeter daily, and that his living quarters were 100 to 300 yards from the perimeter fence. The AOJ had already made favorable findings of diagnoses of CAD, diabetes, hypertension, and prostate cancer. An August 2023 VA examiner separately linked the Veteran's atrial fibrillation to his heart disease.
Why it won: The Board found the Veteran's statements about his duties credible because they were consistent with the circumstances of his service and supported by his personnel records. Resolving reasonable doubt in his favor, the Board found he was as likely as not exposed to herbicides near the base perimeter, which triggered the presumption of service connection for CAD under 38 C.F.R. § 3.309(e).
Fort McClellan herbicide exposure established through expert report and IHP research Citation A26038330 (April 23, 2026), Direct Review docket
The record: The Veteran, a corrections NCO who trained at Fort McClellan, said he observed grounds crews spraying chemicals and smelled them in the air. His representative submitted a detailed Informal Hearing Presentation with a federal Environmental Baseline Survey documenting herbicide use and storage at the base, and a report from Dr. H.M., an environmental scientist, concluding it was more likely than not that anyone stationed at Fort McClellan during the relevant years was exposed to the same herbicide agents used in Vietnam. The AOJ had not developed this theory at all.
Why it won: The Board found the evidence was at least in approximate balance on exposure, given the extensive research and expert report against an AOJ record that contained no analysis of the issue. Once exposure was conceded on a facts-found basis, CAD was presumptively connected under 38 C.F.R. § 3.309(e) because there was no clear and convincing evidence to the contrary.
CAD granted as secondary to PTSD through post-service tobacco use Citation A26038307 (April 23, 2026), Evidence Submission docket
The record: The Veteran argued his service-connected PTSD caused him to smoke heavily after service, and that this tobacco use caused his COPD, hypertension, and CAD. The Veteran and his brother gave competent, credible lay statements about his symptoms and history. A December 2025 private doctor's opinion, which the Board found adequate under Nieves-Rodriguez, cited medical literature linking PTSD to heavier and more persistent smoking, and linked smoking to cardiovascular disease. There was no VA opinion contradicting this theory.
Why it won: Direct service connection for tobacco use itself is barred by law, but secondary connection is allowed where a service-connected disability caused the tobacco use and that tobacco use was a substantial factor in the secondary disability. The Board found the private opinion, lay statements, and treatment records all consistent and probative, and granted CAD on that secondary tobacco-use theory.
Perimeter mechanic duties at U-Tapao support non-PACT herbicide grant Citation A26038036 (April 23, 2026), Hearing docket
The record: The Veteran testified at a Board hearing that as a vehicle mechanic he went to the base perimeter at U-Tapao 3 to 5 times a week, within 10 feet of the perimeter fence, to repair broken-down vehicles. This case came back to the Board after a Court-ordered remand because an earlier decision had only granted service connection effective under the PACT Act, which would have provided no retroactive benefit since the Veteran filed before the Act's enactment.
Why it won: The Board found the Veteran's testimony consistent with his MOS as a vehicle mechanic and therefore credible. It conceded herbicide exposure on a facts-found basis under old M21-1 guidance for Thailand perimeter duty, which allowed the grant to be effective earlier than the PACT Act would allow.
Direct grant for heart disease tied to Gulf War toxic exposures Citation A26037867 (April 22, 2026), Hearing docket
The record: The Veteran described in-service exposure to oil well fires, burning waste, and diesel fumes during Operation Desert Storm, and a heart attack at age 42 requiring stent placement. Multiple private letters, including one stating the cardiac complications "may indeed be linked to the cardiopulmonary disorders brought on by the original fire exposures," supported a connection. A November 2010 VA examiner had found the coronary artery disease "less likely than not" related to environmental exposure, citing other risk factors.
Why it won: The Board found both the positive private opinions and the negative VA opinion probative, creating an approximate balance of evidence. It weighed the Veteran's competent and credible lay testimony about his symptoms and exposures alongside the private opinions' citations to medical literature, and resolved doubt in the Veteran's favor to grant the claim.
Why These Claims Get Denied
Beyond the general "no nexus" and "no qualifying exposure" reasons covered above, a few specific denial patterns show up often enough in published decisions to call out on their own.
- A confirmed diagnosis with no connection to service. Having heart disease, even a clearly documented case, is not enough by itself. VA has conceded the diagnosis and still denied the claim where nothing in the record tied it to service or to a service-connected condition.
- An exposure story the record does not support. A claimed period of qualifying herbicide exposure that conflicts with the veteran's documented service history, or with an earlier statement denying such exposure, has been found not credible and denied. The account has to match what the service and medical records actually show.
- A "could have" opinion instead of a reasoned nexus. A medical opinion stating only that service "could have" caused the heart disease, without walking through the reasoning, has been found too weak to carry a claim. VA looks for an opinion stating the link is at least as likely as not, supported by an explanation.
- Conceded exposure with no medical link to the specific disease. Even where VA accepts that a veteran was exposed to fuels, oils, solvents, or another toxic substance, the claim can still be denied if the examiner attributes the heart disease to other factors, such as hypertension, diabetes, or smoking, instead. Accepted exposure still needs a medical opinion tying it to the heart disease itself.
- A heart attack during off-duty time with no proof it happened on qualifying duty. To count, a heart attack generally has to occur during a qualifying period of active duty, active duty for training, or inactive duty training. A heart attack that happened off duty, for example at home after a personal run, has been found not to qualify as an in-service event.
- A long gap with no records connecting the disease back to service. Waiting decades to see a cardiologist, with no records of heart symptoms within the period closely following service, undercuts a continuity-of-symptoms argument and has been a factor in denials.
DC 7005 Rating Levels
Diagnostic code 7005 has no rating rows of its own. It is rated under the General Rating Formula for Diseases of the Heart at 38 CFR 4.104. The four levels below are reproduced verbatim from the current formula. Each level is reached by the MET workload that produces heart failure symptoms, and the 30 percent and 10 percent levels add an alternate route that does not depend on a measured MET number.
Go deeper: open the full coronary artery disease breakdown- What the VA measures at your C&P exam
- Evidence that has won at the Board
- Inside the rater's playbook: grant, denial, and remand rates
- Secondary condition map
There are three ways to reach a single level. The 30 percent level can be earned either by a measured workload of 5.1 to 7.0 METs OR by imaging that confirms cardiac hypertrophy or dilatation, even if the MET workload is higher. The 10 percent level can be earned either by a workload of 7.1 to 10.0 METs OR simply by the fact that continuous medication is required to control the heart disease. This medication route at 10 percent is the floor for a veteran whose CAD is well controlled on daily heart medication.
A 100 percent evaluation is also assigned for a period of three months following hospital treatment for a documented heart attack (myocardial infarction), separate from the MET-workload rows above.
The table below summarizes the two non-MET routes that often get overlooked.
| Level | Alternate route (no MET number needed) |
|---|---|
| 100% | Three months immediately following hospital treatment for a documented heart attack (myocardial infarction). |
| 30% | Cardiac hypertrophy or dilatation confirmed by echocardiogram, MUGA scan, or cardiac MRI. |
| 10% | Continuous medication required for control of the heart disease. |
Notes from the regulation:
- Note 1: Cor pulmonale, a form of secondary heart disease, is evaluated as part of the pulmonary (lung) condition that causes it, not separately under the heart formula.
- Note 2: One MET is the energy cost of standing quietly at rest. When a laboratory exercise test cannot be done for medical reasons, a medical examiner may estimate the MET level at which symptoms develop, supported by specific examples such as slow stair climbing or shoveling snow.
- Note 3: Heart failure symptoms include, but are not limited to, breathlessness, fatigue, angina, dizziness, arrhythmia, palpitations, or syncope.
- The 7005 Note: If non-service-connected arteriosclerotic heart disease is superimposed on service-connected valvular or other non-arteriosclerotic heart disease, the rater requests a medical opinion as to which condition is causing the current signs and symptoms.
Pyramiding and Rating Separately
The VA's pyramiding rules prevent paying twice for the same symptoms. For heart disease, the rule that surprises many veterans is that hypertension is rated separately from heart disease. Note 3 to 38 CFR 4.104 directs that hypertension (DC 7101) be evaluated separately from hypertensive heart disease and from other types of heart disease, including ischemic heart disease such as CAD. A veteran can hold a percentage for CAD under 7005 and a separate percentage for hypertension under 7101 at the same time.
Within heart disease itself, however, the same symptoms cannot drive two ratings. Coronary artery disease and another heart condition are not stacked on the same MET workload. The 7005 Note also addresses an overlap: if non-service-connected arteriosclerotic heart disease is superimposed on a service-connected non-arteriosclerotic heart condition, the rater requests a medical opinion to sort out which condition is producing the current symptoms.
One more separate-rating point: erectile dysfunction that flows from CAD is its own ratable condition under code 7522 and adds special monthly compensation under SMC-K. That is not pyramiding, because ED and the heart disease are distinct disabilities with distinct effects.
Common Mistakes
The errors the Board's decisions surface most often:
- Confusing ischemic heart disease with hypertension or peripheral vascular disease: the 3.309(e) presumptive covers ischemic heart disease (CAD), but it specifically excludes hypertension and peripheral manifestations of arteriosclerosis, which are separate conditions under different codes.
- Expecting the rating to hinge on ejection fraction: the current 38 CFR 4.104 formula is MET-based, with an echocardiogram hypertrophy or dilatation route at 30 percent and a continuous-medication route at 10 percent. Ejection fraction rows were removed in 2021, so a high ejection fraction does not by itself defeat a MET-based rating.
- Going to the C&P exam with no recent exercise stress test: without a measured MET workload at which heart failure symptoms appear, the file lacks the core data point the rating depends on.
- Assuming the Agent Orange presumption applies without establishing exposure or a diagnosis: the presumption needs both qualifying herbicide exposure (eligible location and dates) and a confirmed current CAD or ischemic heart disease diagnosis in the record.
- Filing a direct claim with no nexus opinion: "no nexus" is the leading dispositive denial reason for DC 7005 in published BVA decisions, and a private nexus opinion is the strongest evidence type when the presumption does not apply.
- Pursuing only a direct theory: overlooking secondary pathways (CAD secondary to service-connected diabetes, hypertension, or sleep apnea) can leave a viable route unused.
- Not claiming downstream secondaries: erectile dysfunction that flows from CAD is separately ratable and opens an SMC-K pathway that is easy to miss.
- Letting your account of dates, places, or symptoms shift between statements. VA weighs credibility. Statements that stay consistent with service and medical records support a claim; accounts that conflict with earlier records have been a reason for denial.
Do's and Don'ts
A condensed version of everything above, in the order it actually matters when you sit down to build your file.
- Check whether your heart disease qualifies for the Agent Orange presumption before building a direct-connection case from scratch.
- Get a VA or private record naming your current coronary artery disease or ischemic heart disease diagnosis into the file.
- If you served in Vietnam, on or near a covered Thailand base, or near the Korea DMZ, gather service records or write a clear, consistent statement placing you there.
- If your claim is not presumptive, ask whether the heart disease is secondary to a service-connected condition like hypertension or diabetes.
- Get a nexus opinion that explains its reasoning and addresses other possible causes, not a bare letter saying service "could have" caused it.
- Keep your account of dates, places, and exposures consistent across every statement, exam, and record.
- Track your METs and ejection fraction if you're already service connected and are due for a rating review.
- Claim downstream secondaries, such as erectile dysfunction, that flow from your heart disease.
- If you were denied before, file a Supplemental Claim with new and relevant evidence rather than starting over.
- Don't assume a diagnosis alone wins the claim, you still need the connection to service or to a service-connected condition.
- Don't give an exposure account your service records don't support, an inconsistent story has been found not credible on its own.
- Don't rely on a nexus opinion that only says service "could have" caused it, VA looks for reasoning, not a bare conclusion.
- Don't assume any toxic exposure guarantees a win, an examiner can still attribute the disease to hypertension, diabetes, or smoking instead.
- Don't count an off-duty heart attack as an in-service event without proof it happened during qualifying duty.
- Don't wait decades to seek treatment and then argue continuity with no records to back it up.
- Don't expect ejection fraction to decide your rating, the current formula runs on MET workload.
- Don't overlook the secondary pathways, a direct-only theory can leave a viable route on the table.
How the MET Rating Works (and Why Ejection Fraction Is No Longer a Rating Row)
The most important thing to understand about a DC 7005 rating is that it runs on METs, not on symptoms and not on ejection fraction. A MET (metabolic equivalent) is a unit of physical workload. Under 38 CFR 4.104, Note 2, one MET is defined as the energy cost of standing quietly at rest (an oxygen uptake of 3.5 milliliters per kilogram of body weight per minute). The rating asks a single question: at what level of physical exertion (measured in METs) do heart failure symptoms appear?
Note 3 to the formula defines what counts as a heart failure symptom for rating purposes. The list includes, but is not limited to, breathlessness, fatigue, angina (chest pain), dizziness, arrhythmia, palpitations, or syncope (fainting). The lower the MET workload that triggers any of these, the higher the rating.
Quick Checklist Before You File
Bring these together before you submit anything.
- A VA or private record that names your current coronary artery disease or ischemic heart disease diagnosis.
- Whether you served in Vietnam, on or near a covered Thailand base (1962 to 1976), or near the Korea DMZ during the covered dates.
- If you did, service records or a clear, consistent statement placing you there.
- If your claim is not presumptive, whether heart disease is secondary to a service-connected condition like hypertension or diabetes.
- A medical nexus opinion that explains its reasoning, not just a letter saying service "could have" caused it.
- Your account of dates, places, and exposures kept consistent across every statement and record.
- If you're already service connected, your MET workload and ejection fraction for rating, and awareness of the effective-date and reduction rules.
- If you were denied before: new and relevant evidence for a Supplemental Claim, not just a repeat of what was already considered.
For the mechanics of actually submitting the claim, see the Standard Claim Guide and the Fully Developed Claim Guide (filing with all your evidence up front can speed up the decision).
The Claims Process, Step by Step
Once you file, your claim moves through a series of hand-offs. Understanding who does what helps you know who to contact, and what to expect, at each stage.
- You file the claim. Directly with VA, through VA.gov, or with the help of an accredited representative. If you have not yet gathered your evidence, filing an Intent to File can lock in an earlier potential effective date while you do.
- VA acknowledges the claim and assigns it for development. A Veteran Service Representative (VSR) is assigned to gather your service treatment records, VA and private medical records, and any other evidence needed, including proof of qualifying herbicide exposure if you're pursuing the presumption.
- The VSR orders a Compensation & Pension (C&P) exam if one is needed. Presumptive claims sometimes skip a nexus-focused exam once exposure and diagnosis are established; direct and secondary claims typically require one.
- The C&P exam is conducted. By a VA clinician or a contracted examiner, who completes the Ischemic Heart Disease Disability Benefits Questionnaire (DBQ), documenting the diagnosis, the MET workload, and, where relevant, a nexus opinion.
- The file goes to a Rating Veteran Service Representative (RVSR), the "rater." The rater reviews the complete file, including the exam results, and decides whether service connection is warranted and at what percentage.
- A senior reviewer may review the decision before it's finalized, depending on the complexity of the claim.
- VA issues the decision letter. This states whether the claim is granted or denied, the rating percentage if granted, the effective date, and the reasons behind the decision.
- If you disagree, you choose an appeal lane. Higher-Level Review, Supplemental Claim, or a Board appeal, covered later in this guide.
Who's who: VSO vs. VSR vs. Rater vs. C&P Examiner
Your VSO
An accredited representative from a veterans service organization, or an accredited attorney or claims agent. Not a VA employee. Helps you prepare, gather evidence, and file, and can represent you through an appeal. Has no authority to decide your claim.
VSR (Veteran Service Representative)
VA staff who "develops" your claim: requests records, schedules the C&P exam, and assembles the file. Does not decide the rating.
Rater (RVSR)
VA staff who reviews the completed file and makes the actual decision, service connection or denial, and the percentage. This is the person whose judgment the decision letter reflects.
C&P Examiner
A VA clinician or a contracted medical examiner who conducts the exam and completes the DBQ. Documents findings, the MET workload, and, where asked, a nexus opinion. Does not decide the claim.
For the full walkthrough of every stage with more detail, see Inside Your Claim and Claim Stages.
Diagnostic Tests and Your C&P Exam
The primary exam document for DC 7005 is the Ischemic Heart Disease Disability Benefits Questionnaire (VA Form 21-0960A-1), which covers coronary artery disease and the residuals of a heart attack. See the DBQ guide for how these forms work generally, including whether a private DBQ completed by your own doctor can be submitted instead of relying solely on a VA exam. For a full walkthrough of what to expect at the exam itself and how to prepare, see the C&P Exam Prep Guide.
The tests and measurements that appear on these exams, and what each one establishes, are catalogued below.
- Exercise stress test (treadmill test): measures the MET workload at which heart failure symptoms (breathlessness, fatigue, angina, dizziness, arrhythmia, palpitations, or syncope) develop. This is the central rating metric under 38 CFR 4.104.
- Examiner-estimated METs: when an exercise test cannot be done for medical reasons, Note 2 allows the examiner to estimate the MET level using specific activity examples such as slow stair climbing or shoveling snow.
- Echocardiogram (or MUGA scan or cardiac MRI): documents cardiac hypertrophy or dilatation, the alternate route to the 30 percent level.
- Cardiac catheterization / coronary angiography: confirms the coronary artery disease diagnosis and the degree of arterial blockage.
- Electrocardiogram (EKG) and Holter monitoring: detect ischemia, prior heart attack, and arrhythmia.
- Ejection fraction (LVEF): still routinely reported to describe severity, even though it is no longer a stated rating-row threshold in the current formula.
- Lipid panel, cardiac biomarkers, and medication records: support the diagnosis and document continuous cardiac medication, the basis for the 10 percent medication route.
Reading Your Decision Letter, and What to Do If Denied
Your decision letter has two parts: a narrative section explaining the reasoning (often called "reasons and bases"), and a codesheet showing the actual rating percentage, the effective date, and the diagnostic code used. See the Reading Your Decision Letter Guide for how to find and interpret each part, or use the Letter Interpreter tool to upload your own letter and get a plain-English breakdown.
If your claim is denied, or the rating is lower than you expected, you have three main lanes:
- Supplemental Claim: refile with new and relevant evidence, such as a new nexus opinion, a corrected exposure statement, or an updated stress test. See Supplemental Claim Guide.
- Higher-Level Review (HLR): a senior reviewer looks at the same evidence again for a difference of opinion, no new evidence is added. See HLR Guide.
- Board Appeal: your case goes to a Veterans Law Judge at the Board of Veterans' Appeals, with options for a direct review, an evidence docket, or a hearing. See Board Appeal Guide.
Not sure which lane fits your situation? See the Appeals decision guide for a side-by-side comparison of all three.
After You Win: Maintaining Your Rating
A grant is not always the end of the story. Keep your treatment consistent, continued follow-up with a cardiologist, updated stress tests, and medication records, protects you if VA schedules a future reexamination. If VA proposes to reduce a rating, it has to show the heart disease actually improved in the veteran's daily functioning; a shorter or less thorough exam is not enough by itself to justify a cut. Not every rating gets reexamined; understand when a rating becomes protected from future review (including Permanent and Total status) and what to do if VA proposes to reduce it. See Protect Your Rating and Future Reexaminations for the specifics.
If your coronary artery disease worsens after the initial grant, for example a drop in your MET workload or a new complication, you can file for an increased rating. See the Rating Increase Guide.
Common Secondary Conditions
Coronary artery disease sits in the middle of a chain. It is caused by some conditions and it causes others. The Board's secondary-claim data show both directions clearly, and each rate below is a grant rate paired with its sample size from published BVA decisions.
Conditions that cause CAD (CAD claimed secondary TO them)
We found each bar is the published BVA grant rate for CAD claimed secondary to that condition, with the number of decisions below it. This is the "ways to connect via another condition" list:
Conditions that CAD causes (claimed secondary to CAD)
We found each bar is the published BVA grant rate for that condition claimed secondary to CAD:
Quick Reference Tables
Service Connection and Secondary Pathways
| Pathway | Mechanism | Evidence Needed |
|---|---|---|
| Agent Orange presumptive (38 CFR 3.309(e)) | Qualifying herbicide exposure presumed to cause ischemic heart disease | Current CAD/IHD diagnosis + qualifying service location and dates |
| Direct service connection | Disease began during or was caused by an in-service event or exposure | Diagnosis + in-service event + medical nexus opinion |
| Secondary to diabetes | Diabetes damages blood vessels over time, contributing to CAD | Nexus opinion linking service-connected diabetes to the heart disease |
| Secondary to hypertension (DC 7101) | Long-standing high blood pressure accelerates arterial disease | Nexus opinion linking service-connected hypertension to the heart disease |
| Secondary to sleep apnea (DC 6847) | Repeated oxygen drops strain the cardiovascular system | Nexus opinion linking service-connected sleep apnea to the heart disease |
From Filing to Decision: Who Does What
| Role | Does | Decides your rating? |
|---|---|---|
| VSO / accredited representative | Helps prepare, gather evidence, and file; represents you on appeal | No |
| VSR | Develops the claim: orders records and the C&P exam | No |
| C&P Examiner | Conducts the exam, completes the DBQ, records the MET workload, may give a nexus opinion | No / but has a strong impact |
| Rater (RVSR) | Reviews the full file and decides service connection and percentage | Yes |
Frequently Asked Questions
Is coronary artery disease an Agent Orange presumptive condition?
Does my ejection fraction decide my rating?
What is a MET, and what if I am too sick to take a stress test?
Can I be rated for both coronary artery disease and high blood pressure?
I have erectile dysfunction from my heart disease. Is that worth claiming?
My CAD claim was denied for "no nexus." What does that mean?
When does my effective date start for a presumptive Agent Orange heart disease grant?
What if VA tries to reduce my heart disease rating?
Related Tools and Guides
Sources
- 38 CFR 4.104, DC 7005 and 7006, the General Rating Formula for Diseases of the Heart
- 38 CFR 3.303, basic rules for service connection
- 38 CFR 3.310, secondary service connection
- 38 CFR 3.307 and 3.309(e), presumptive service connection for herbicide/Agent Orange exposure, including ischemic heart disease
- 38 CFR 3.102, benefit of the doubt; 38 CFR 3.6, active duty, active duty for training, and inactive duty training
- 38 CFR 3.400 and 3.114, effective dates and liberalizing laws; 38 CFR 3.344, rating reductions
- 38 USC 1110, 1116, 1116B, and 1131, service connection and herbicide presumptions; 38 USC 5107(b), benefit of the doubt
- PACT Act, Pub. L. No. 117-168 (2022), expanded herbicide presumptions to Thailand and the Korea DMZ and added covered conditions
- VA Public Health, ischemic heart disease and Agent Orange
- VA.gov, Agent Orange exposure eligibility
- 38 CFR 3.350, special monthly compensation (SMC-K)