VA Asthma Claims Guide
Bronchial asthma is one of the respiratory conditions most often tied to military service, and the rating rules under diagnostic code 6602 reward veterans who understand them. This guide walks the whole path: how service connection works, how asthma gets connected to your service (directly, through the PACT Act burn pit presumptive, or secondary to another condition), how the DC 6602 rating actually runs on two separate measures, your lung-function numbers and your medications, what evidence you need, why these claims get denied, a checklist before you file, what the claims process looks like step by step, how to read your decision letter, and what to do whether you win or you're denied.
 One-page guide: Asthma Claim in One Page
Five-part visual guide to asthma claims covering service-connection routes, pulmonary-function tests, medication and exacerbation evidence, DC 6602 ratings, and a filing checklist. Opens the full-size chart, free to save or print.
One-page guide: Asthma Claim in One Page
Five-part visual guide to asthma claims covering service-connection routes, pulmonary-function tests, medication and exacerbation evidence, DC 6602 ratings, and a filing checklist. Opens the full-size chart, free to save or print.
What the VA Counts as Bronchial Asthma
For VA purposes, bronchial asthma is rated under 38 CFR 4.97, diagnostic code 6602. Asthma is a chronic disease of the airways that causes them to narrow, swell, and produce extra mucus, leading to wheezing, shortness of breath, chest tightness, and coughing. The condition is variable: it can be quiet for stretches and then flare into an attack triggered by allergens, exercise, cold air, infection, or irritants such as smoke or dust.
The objective measure
Spirometry (a breathing test) produces two numbers the rating table uses: FEV-1, the percent of air you can forcefully exhale in the first second compared to what is predicted for your age and size, and the FEV-1/FVC ratio, which compares that first-second volume to your total forced exhale.
The treatment measure
The kind and amount of medicine you need is a separate path to the same percentages. Daily bronchodilators or inhaled anti-inflammatories, monthly physician visits for flare-ups, and systemic (oral or injected) steroids each map to a specific rating level on their own.
Symptoms Recorded in Granted Asthma Decisions
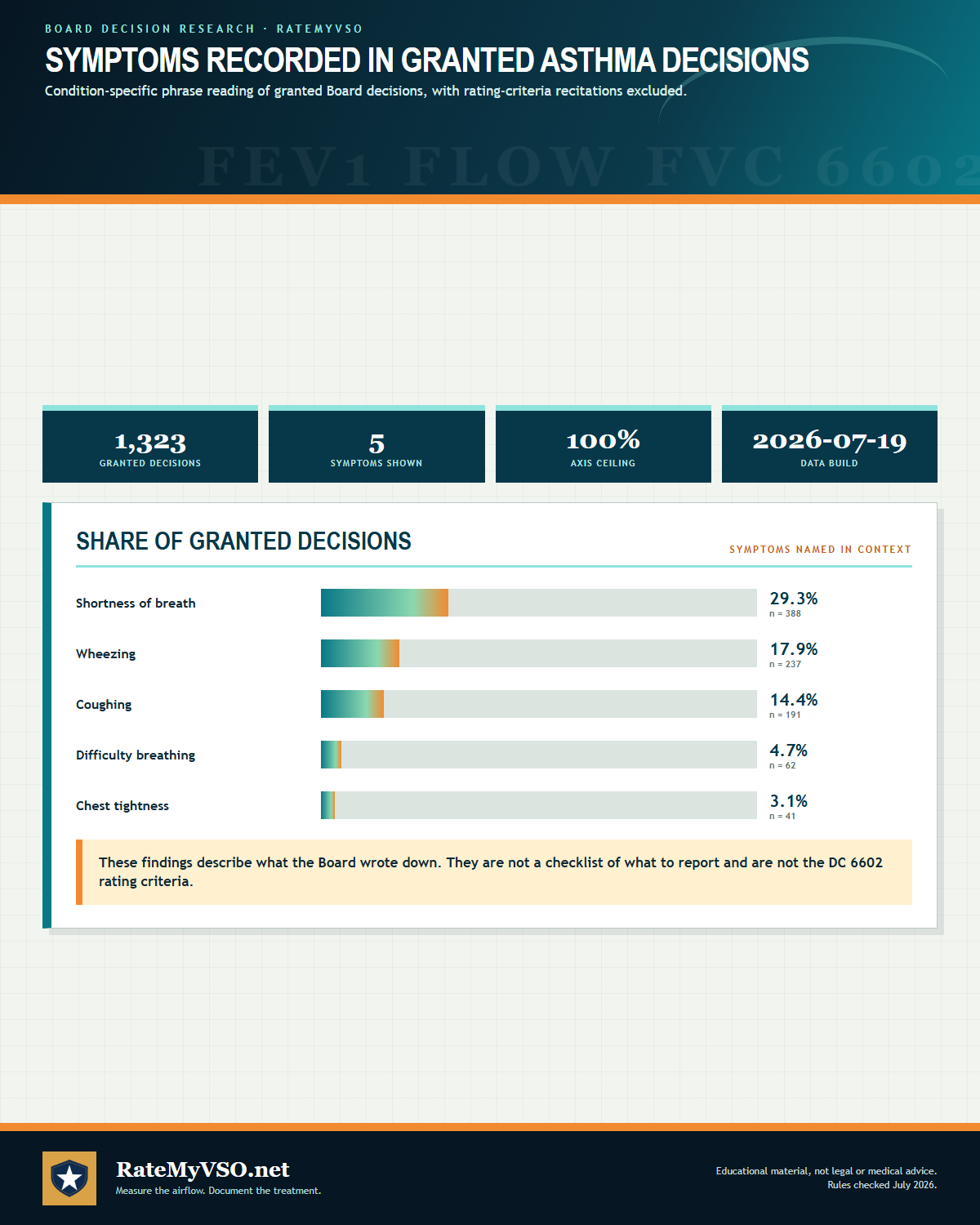
We analyzed 1,323 granted Board decisions involving asthma for symptoms named in sentences about the condition (rating-criteria recitations excluded). Descriptive of the published record, what the Board wrote down, not a checklist of what to report.
Detected by phrase-reading the decision text with condition-specific vocabularies. Source: Board of Veterans' Appeals decisions, RateMyVSO analysis.
 One-page guide: Symptoms Recorded in Granted Asthma Decisions
Bar chart of the symptoms most often recorded across 1,323 granted asthma Board decisions, with rating-criteria recitations excluded. Opens the full-size chart, free to save or print.
One-page guide: Symptoms Recorded in Granted Asthma Decisions
Bar chart of the symptoms most often recorded across 1,323 granted asthma Board decisions, with rating-criteria recitations excluded. Opens the full-size chart, free to save or print.
ICD-10 Diagnosis Codes
The ICD-10 diagnosis codes most commonly used for DC 6602, Asthma, bronchial (the kind on your medical records, decision letter, or C&P exam report). VA rates the disability and its residuals, not the diagnosis itself, so coding can vary.
How Service Connection Works, At a High Level
Before getting into the specific pathways below, it helps to understand the three things every asthma claim ultimately has to show. This is the same basic test that applies to any VA disability claim, just applied to this condition.
- A current diagnosis. A doctor must confirm you have asthma now. This is the cornerstone of the claim under 38 CFR 3.303, and without it the claim fails, even when a presumption would otherwise apply. A VA treatment note documenting an asthma assessment together with a prescribed inhaler can be enough to confirm the diagnosis, even if a later examiner expresses doubt.
- An in-service event, or a service-connected condition behind it. Something that happened or was documented during your service, such as toxic or burn pit exposure or breathing symptoms that started during service, or a disability VA has already service-connected that caused or worsened your asthma.
- A medical nexus. A reason to connect the two, usually a medical opinion. For asthma, this step is often the easiest, because of the presumptions described below: for many Gulf War era and post-9/11 veterans, the law presumes the link, so no nexus opinion is needed at all.
How Bronchial Asthma Gets Service Connected
 One-page guide: Direct Service Connection
Direct asthma denial research across 4,033 classified service-connection denials, split by whether the file was missing a medical nexus, a current diagnosis, or an in-service event, followed by the three required direct-service-connection elements. Opens the full-size chart, free to save or print.
One-page guide: Direct Service Connection
Direct asthma denial research across 4,033 classified service-connection denials, split by whether the file was missing a medical nexus, a current diagnosis, or an in-service event, followed by the three required direct-service-connection elements. Opens the full-size chart, free to save or print.
Direct service connection
Direct service connection requires a current asthma diagnosis, an in-service event, exposure, or onset, and a medical nexus linking the two. We analyzed the published BVA decisions and found the missing link is overwhelmingly the nexus. A private medical opinion moved outcomes sharply: asthma appeals were granted at a markedly higher rate when a private nexus opinion was in the file. Describing when your breathing problems started and that they never stopped matters here too: lay statements that asthma began in service and continued since, especially when matched by service treatment records, can carry a direct claim even without an in-service asthma diagnosis on record.
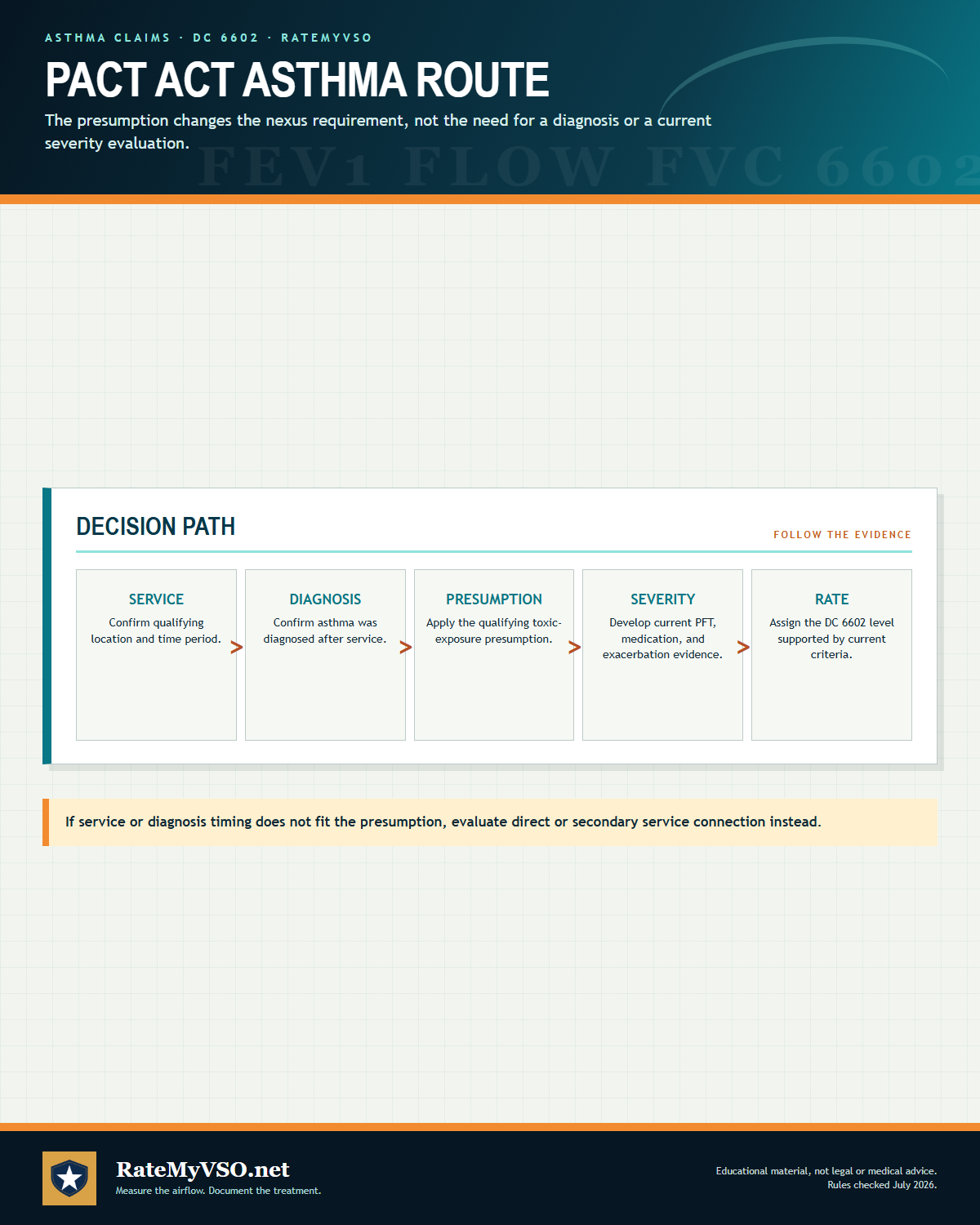 One-page guide: PACT Act Asthma Route
Five-step PACT Act asthma path covering qualifying service, post-service diagnosis, presumption, severity evidence, and rating. Opens the full-size chart, free to save or print.
One-page guide: PACT Act Asthma Route
Five-step PACT Act asthma path covering qualifying service, post-service diagnosis, presumption, severity evidence, and rating. Opens the full-size chart, free to save or print.
Presumptive service connection: the PACT Act burn pit pathway
This is the standout path for many post-1990 veterans, and often the fastest route to a grant. Under the PACT Act, bronchial asthma diagnosed after service is a presumptive condition for veterans with qualifying airborne-hazard or burn pit exposure. For a presumptive claim, you do not have to prove a nexus. Qualifying service does the linking work. VA.gov lists asthma among the burn pit and other airborne-hazards presumptive conditions, alongside chronic bronchitis, COPD, chronic rhinitis, chronic sinusitis, constrictive or obliterative bronchiolitis, emphysema, granulomatous disease, interstitial lung disease, pleuritis, pulmonary fibrosis, and sarcoidosis.
Separately, under 38 CFR 3.320, asthma is presumed service connected for Persian Gulf War veterans presumed exposed to fine particulate matter, and it can be granted even if the asthma appeared after service. Both presumptions still require a current asthma diagnosis in the file; a veteran who was once told he had asthma but was actually diagnosed with COPD does not qualify, because even a presumption needs the current diagnosis to be asthma specifically. And conceded exposure by itself is not an automatic win outside these presumptions: where a medical opinion in the file finds no link, for example characterizing the asthma as allergy-induced with a remote onset unrelated to the exposures, the claim can still be denied even with exposure conceded.
Qualifying service generally means the Gulf War theater (on or after August 2, 1990, including Iraq, Kuwait, Saudi Arabia, Bahrain, Oman, Qatar, the United Arab Emirates, Somalia, and the airspace above) or post-9/11 service (on or after September 11, 2001, including Afghanistan, Djibouti, Egypt, Jordan, Lebanon, Syria, Uzbekistan, Yemen, and the airspace above). See the burn pit presumptive walkthrough and the VA.gov PACT Act page.
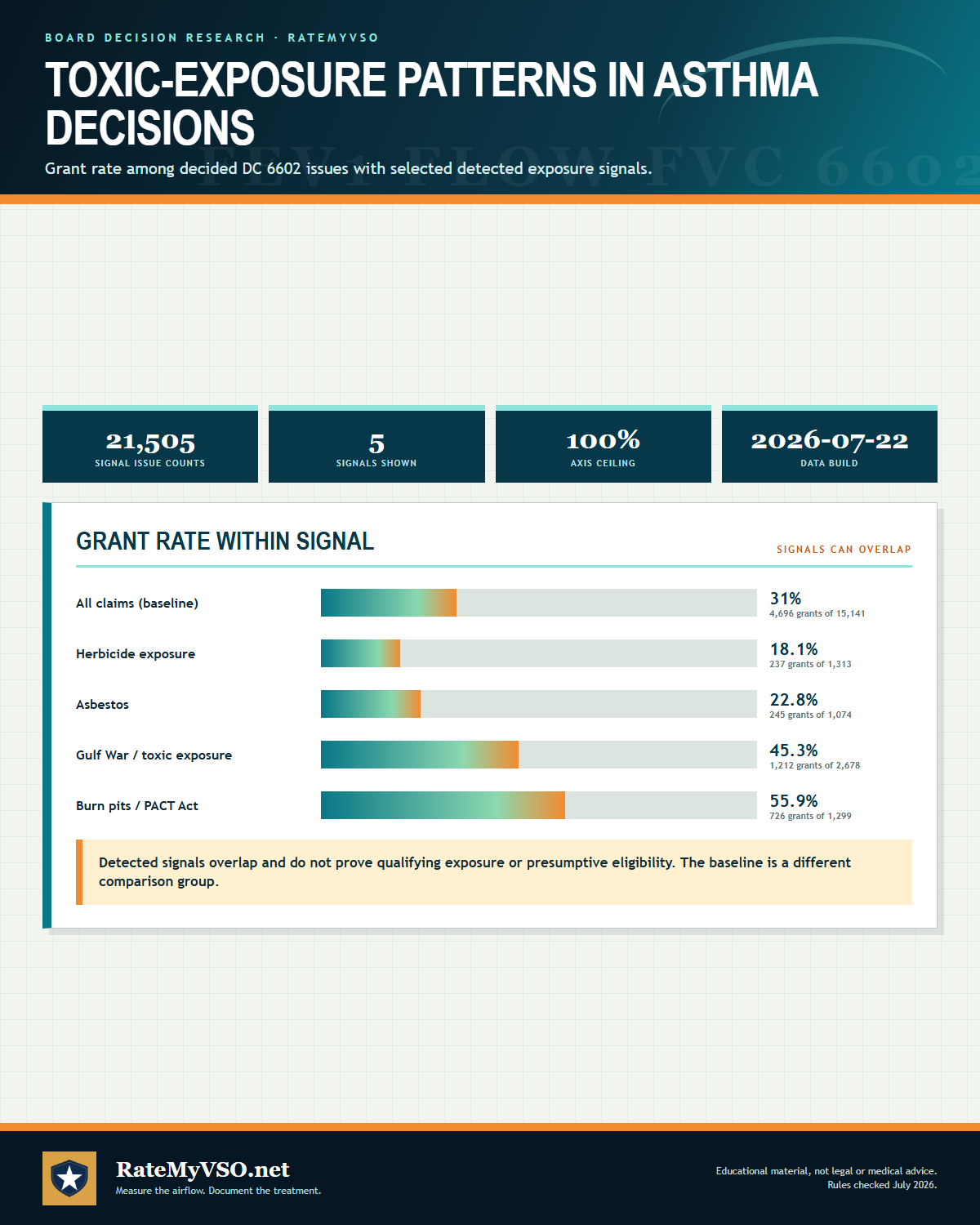 One-page guide: Toxic-Exposure Patterns in Asthma Decisions
Board grant rates by detected toxic-exposure signal across 21,158 decided asthma issues. Opens the full-size chart, free to save or print.
One-page guide: Toxic-Exposure Patterns in Asthma Decisions
Board grant rates by detected toxic-exposure signal across 21,158 decided asthma issues. Opens the full-size chart, free to save or print.
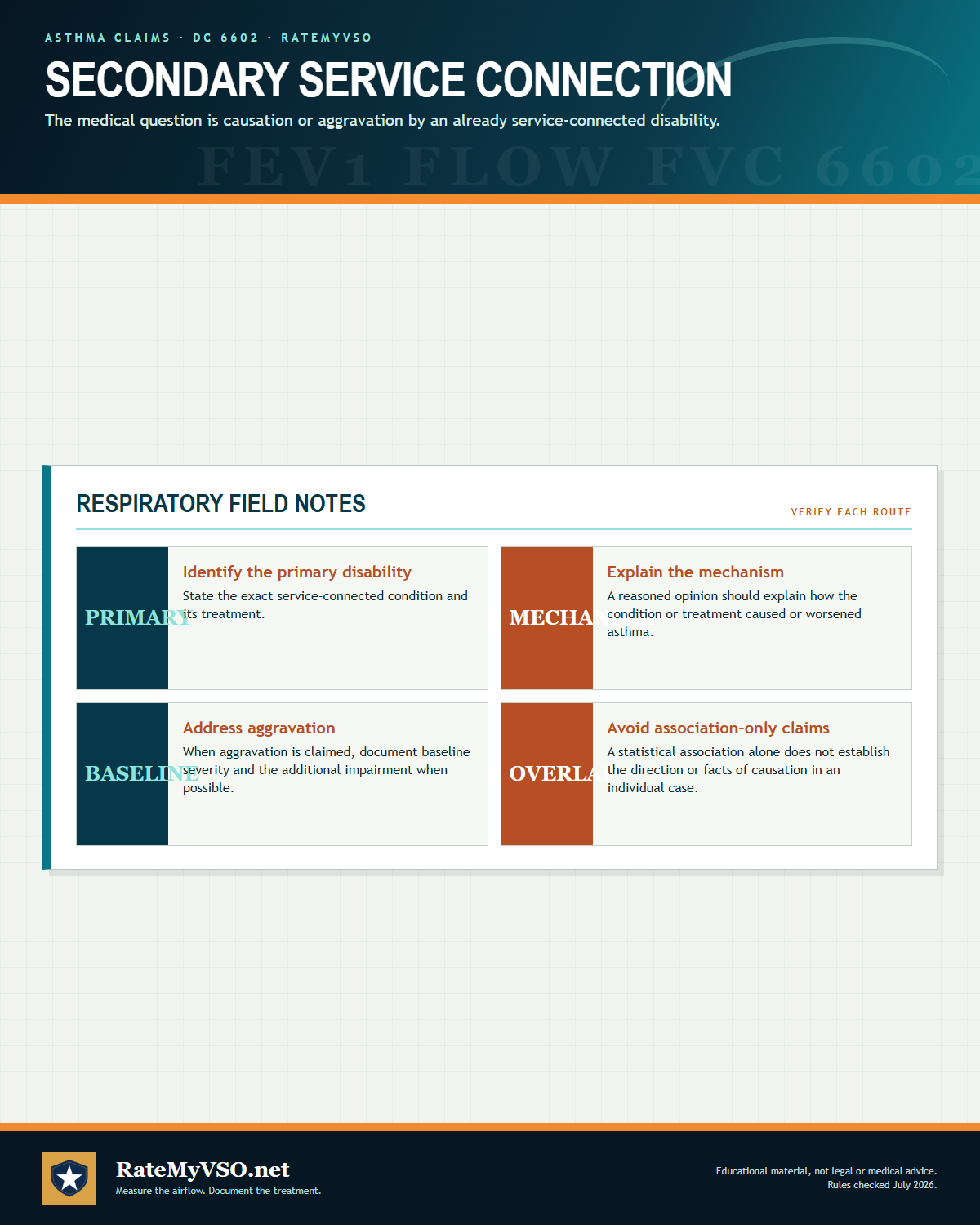 One-page guide: Secondary Service Connection
Secondary service-connection framework covering the primary disability, medical mechanism, aggravation baseline, and association limits. Opens the full-size chart, free to save or print.
One-page guide: Secondary Service Connection
Secondary service-connection framework covering the primary disability, medical mechanism, aggravation baseline, and association limits. Opens the full-size chart, free to save or print.
Secondary to service-connected rhinitis or sinusitis (the "united airway" theory)
This is the strongest secondary pathway in the BVA data. Under the "united airway" concept, the upper airway (nose and sinuses) and lower airway (bronchi) are treated as one connected system, so chronic rhinitis or sinusitis can cause or aggravate asthma. In published decisions, asthma claimed as secondary to allergic or vasomotor rhinitis (DC 6522) is the standout secondary theory, and asthma is also claimed as secondary to sinusitis (DC 6510). A secondary claim under 38 CFR 3.310 turns on a medical opinion linking the service-connected upper-airway condition to the asthma. See secondary conditions and nexus letters.
The GERD-asthma association
Gastroesophageal reflux disease and asthma frequently co-occur and can aggravate one another. Refluxed acid can irritate the airway and worsen asthma symptoms. Asthma is also claimed as secondary to GERD (DC 7206). The pathway runs in both directions in the data, which is covered in the secondary section below. See the GERD claims guide.
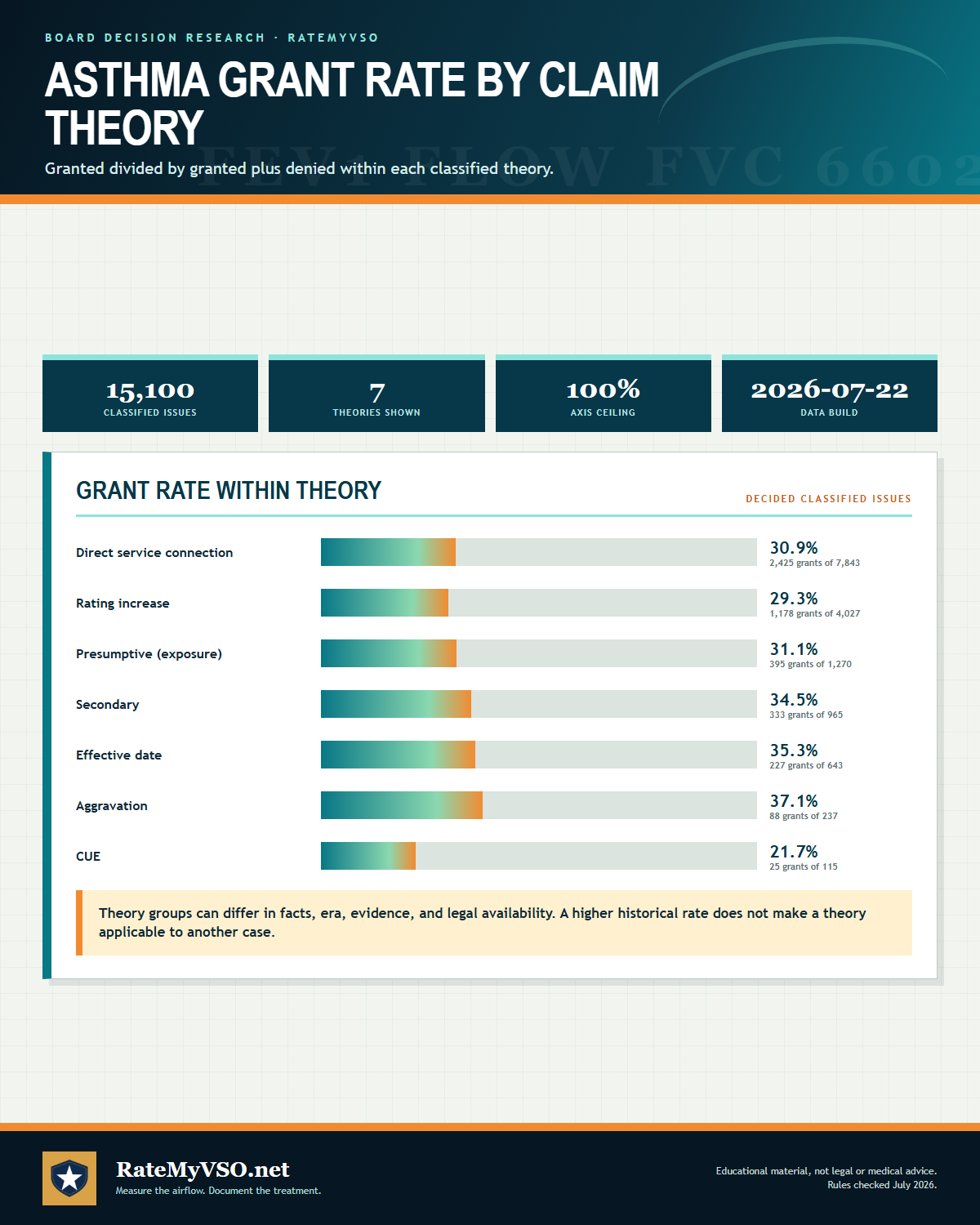 One-page guide: Asthma Grant Rate by Claim Theory
Board grant rates by claim theory across 14,842 decided classified asthma issues. Opens the full-size chart, free to save or print.
One-page guide: Asthma Grant Rate by Claim Theory
Board grant rates by claim theory across 14,842 decided classified asthma issues. Opens the full-size chart, free to save or print.
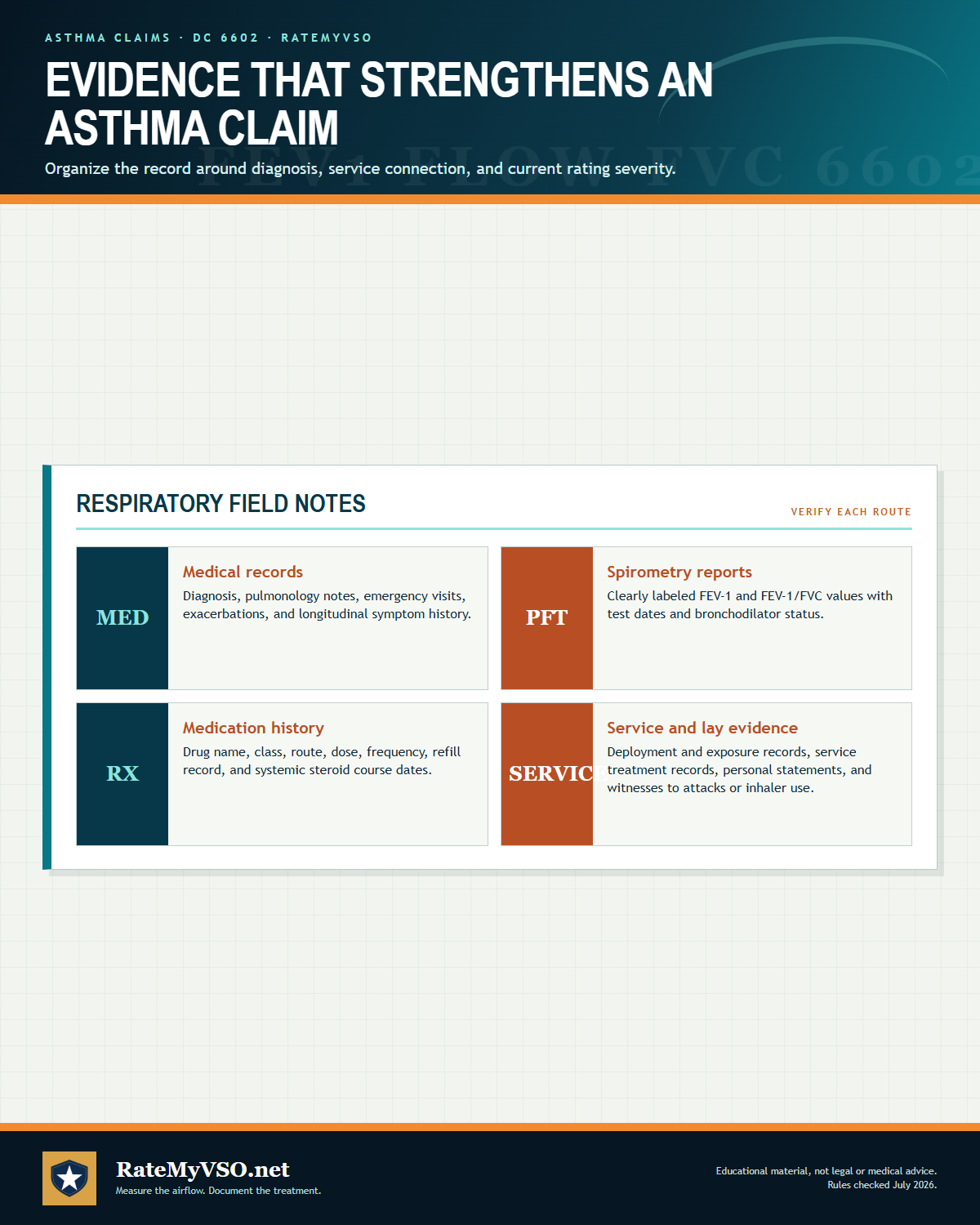 One-page guide: Evidence That Strengthens an Asthma Claim
Medical, spirometry, medication, service, and lay evidence that can strengthen an asthma claim. Opens the full-size chart, free to save or print.
One-page guide: Evidence That Strengthens an Asthma Claim
Medical, spirometry, medication, service, and lay evidence that can strengthen an asthma claim. Opens the full-size chart, free to save or print.
Evidence That Wins These Claims
We analyzed the Board's published decisions and found a private medical opinion is the highest-yield evidence for these claims:
Beyond the nexus, the records that carry weight for an asthma claim are the objective and treatment documents the schedule keys on:
- A current diagnosis in writing: a VA or private doctor's note confirming the asthma diagnosis. A VA treatment note assessing asthma together with a prescribed inhaler such as Albuterol has been enough to confirm a diagnosis even when an examiner later expressed doubt.
- Post-bronchodilator pulmonary function tests: a spirometry report that clearly labels pre-bronchodilator and post-bronchodilator FEV-1 and FEV-1/FVC values, so the rater can apply the correct number under 38 CFR 4.96(d).
- The Respiratory Conditions DBQ: the examiner documents FEV-1/FVC, the treatment regimen, attack frequency, and exacerbations on the VA's questionnaire. See the DBQ guide.
- Medication records that name the drug class: records that distinguish an inhaled corticosteroid (30 percent level) from a systemic oral or parenteral steroid (60 to 100 percent levels), and that show how often systemic courses were prescribed. A full medication list and dosing history is the key evidence for a higher rating; one veteran reached a 100 percent rating in part because a private pulmonologist confirmed he was steroid dependent on a high dose of oral prednisone.
- A verified history of asthmatic attacks: required by the 6602 Note when no asthma findings are present at the exam.
- Lay and buddy statements: your own account of when breathing problems started and that they continued, along with statements from people who observed your symptoms during and after service, can carry a claim even without an in-service asthma diagnosis, especially when service treatment records line up with the timeline. Credible lay evidence of continuous symptoms cannot be dismissed just because service records are silent on the issue or old records are unavailable.
Evidence Cited in Published Asthma Decisions
We analyzed 15,249 published Board decisions involving asthma for condition-specific evidence, counting only case-specific mentions (boilerplate recitations excluded). "Favorable" is the share of decisions citing that evidence where every issue was granted or the outcome was mixed; the baseline across all these decisions is 58.4%. Evidence appearing in a decision does not mean it decided the case. Descriptive of the published record, not a prediction.
Detected by phrase-reading the decision text with condition-specific vocabularies. Source: Board of Veterans' Appeals decisions, RateMyVSO analysis.
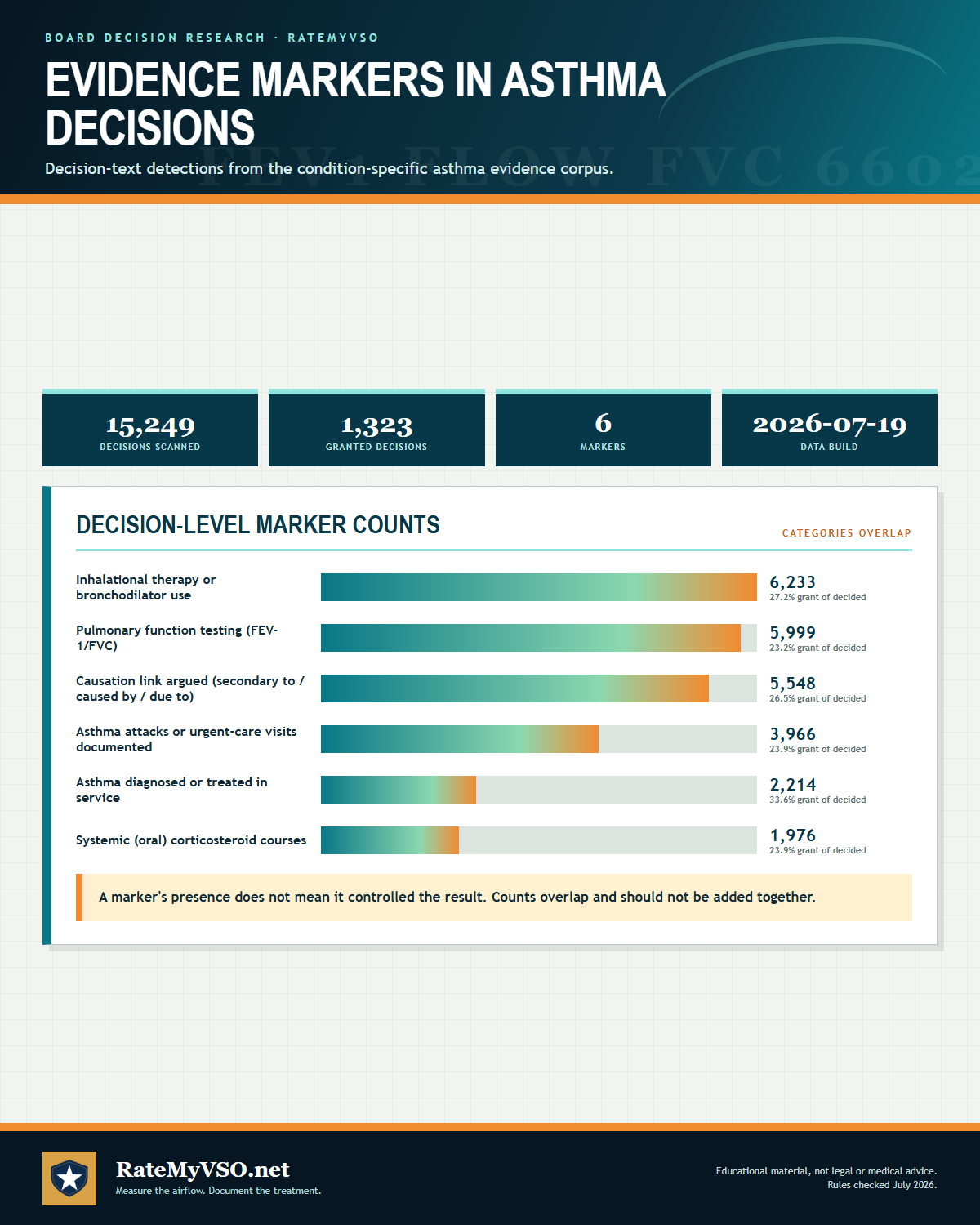 One-page guide: Evidence Markers in Asthma Decisions
Decision-level counts of inhaler, pulmonary-function, causation, exacerbation, in-service onset and systemic steroid markers across 15,249 scanned asthma decisions. Opens the full-size chart, free to save or print.
One-page guide: Evidence Markers in Asthma Decisions
Decision-level counts of inhaler, pulmonary-function, causation, exacerbation, in-service onset and systemic steroid markers across 15,249 scanned asthma decisions. Opens the full-size chart, free to save or print.
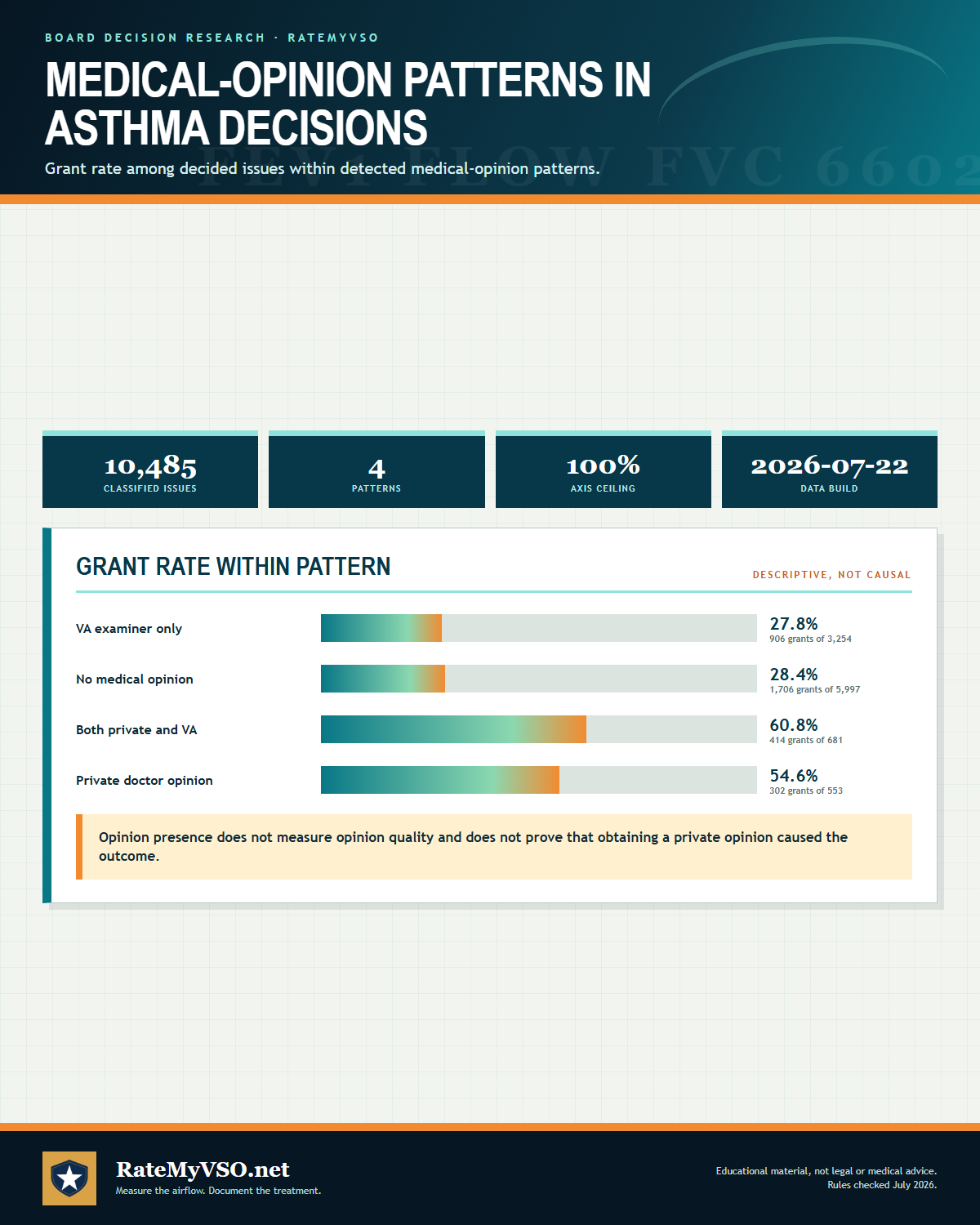 One-page guide: Medical-Opinion Patterns in Asthma Decisions
Board grant rates by detected medical-opinion pattern across 10,742 decided asthma issues. Opens the full-size chart, free to save or print.
One-page guide: Medical-Opinion Patterns in Asthma Decisions
Board grant rates by detected medical-opinion pattern across 10,742 decided asthma issues. Opens the full-size chart, free to save or print.
Board Grants, Dissected
The Board decisions below show several different paths veterans used to win direct service connection for bronchial asthma. Some cases involved asthma that started with no prior history, others involved a preexisting childhood condition that got worse in service, and one case involved a wrongful severance of a rating that had already been granted. What ties these grants together is that the veteran had some combination of credible testimony about when symptoms began, a supportive medical opinion, and a VA opinion that the Board found inadequate or unpersuasive for a specific, identifiable reason. Board decisions are not binding precedent on future cases, but the patterns below repeat often enough to be worth understanding.
Spouse's nurse credentials outweighed two VA exam opinions on anesthesia Citation A26039223 (April 2026), Hearing docket
The record: The veteran had two in-service surgeries and was later diagnosed with asthma and COPD. His spouse, a nurse with over fifteen years of experience, submitted a detailed nexus opinion tying his pulmonary disability to the surgeries and post-surgery care. Two VA opinions from August and September 2019 found against service connection, both reasoning that anesthesia is rarely a causative factor for pulmonary disability.
Why it won: The Board treated the spouse as a medical professional given her nursing background and found her opinion "highly probative." It found that both VA opinions focused narrowly on anesthesia and never addressed the other surgery-related factors the spouse discussed, so neither could negate her opinion. The Board resolved the resulting doubt in the veteran's favor.
Preexisting asthma found not clearly and unmistakably unaggravated by service Citation A26038944 (April 2026), Hearing docket
The record: The veteran's asthma was diagnosed at age five, and his enlistment exam noted it as "not considered disabling." He testified he never had an asthma attack or used an inhaler before service, but needed one after an uptick in symptoms verified in his service treatment records.
Why it won: Because asthma preexisted service, VA had the burden to show by clear and unmistakable evidence that it was not aggravated. The Board found the record showed the veteran was largely asymptomatic for about fifteen years before service and only became symptomatic in service, so VA could not meet that heavy burden. The claim was granted as aggravation of a preexisting condition.
Severance overturned after VA relied on an inapplicable PACT Act framework Citation A26038740 (April 2026), Direct Review docket
The record: VA had granted service connection for asthma, then proposed severance based on a finding that burn pit exposure could not be conceded under the PACT Act. Two earlier VA opinions were internally inconsistent or failed to address the veteran's lay statements about burn pit exposure and destroyed service treatment records. A later August 2025 VA opinion actually found the asthma was at least as likely as not caused by burning trash exposure.
Why it won: The Board explained that the burden for severance is on the government and must be undebatable. Because the PACT Act presumption did not apply to this veteran's era of service, VA's focus on that framework missed the direct service connection theory entirely. With conflicting opinions and one opinion actually supporting the claim, the Board found VA could not meet the clear and unmistakable standard required to sever a rating already granted.
In-service asthma symptoms with continuity found credible despite decades gap in some records Citation A26037551 (April 2026), Hearing docket
The record: The veteran's service treatment records showed a March 1984 asthma notation. He testified he was treated with albuterol during an episode in service and had recurring breathing difficulty afterward, sometimes self-treating rather than seeking formal care.
Why it won: The Board found the veteran competent to report his own respiratory symptoms and found his statements about onset and continuity credible because they were internally consistent and matched the documented in-service treatment. Even though he was not formally diagnosed until after service, the Board found this sufficient because service connection can be granted for a disease diagnosed after discharge when the evidence shows in-service incurrence.
Asthma onset during a period of active duty for training established through lay evidence alone Citation A26036076 (April 2026), Direct Review docket
The record: The Appellant was diagnosed with asthma and treated with medication during basic training. VA found the condition preexisted service based on a report that she used a nebulizer as a child, but she and family members submitted statements denying any childhood respiratory history. The Board found one service record date unreliable due to an apparent typo.
Why it won: The Board found the conflicting lay evidence about pre-service history was credible and that competent lay evidence can be sufficient by itself to establish a claim, without requiring a medical opinion. Because she had not yet achieved "Veteran" status through prior active duty, the Board also had to separately confirm her disability began during her qualifying training period, which the evidence supported.
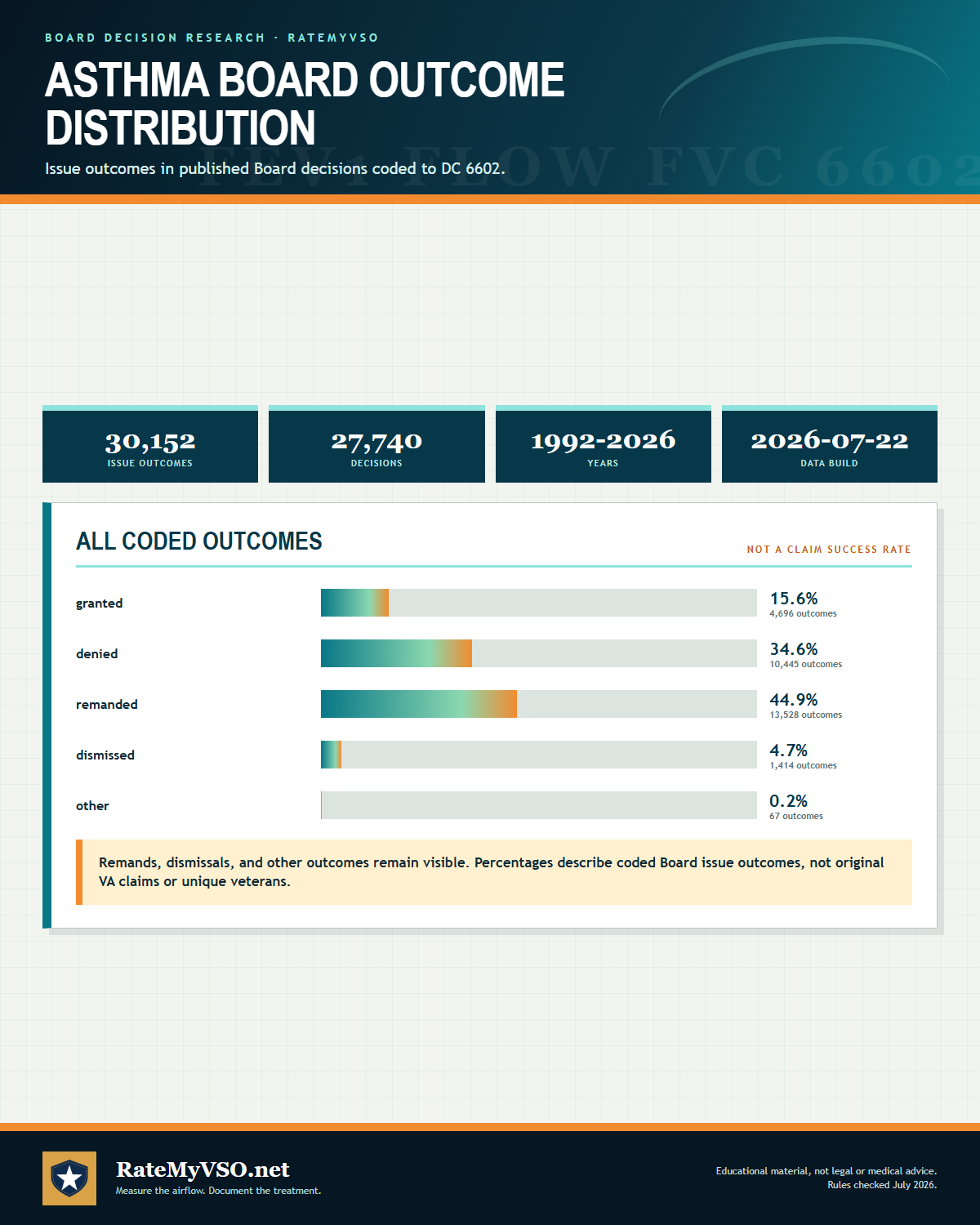 One-page guide: Asthma Board Outcome Distribution
Distribution of grants, denials, remands, dismissals and other coded asthma Board outcomes across 29,661 coded issues from 27,239 decisions. Opens the full-size chart, free to save or print.
One-page guide: Asthma Board Outcome Distribution
Distribution of grants, denials, remands, dismissals and other coded asthma Board outcomes across 29,661 coded issues from 27,239 decisions. Opens the full-size chart, free to save or print.
 One-page guide: Common Reasons Asthma Claims Are Denied
Four common asthma denial categories involving diagnosis, nexus, medication classification, and severity documentation. Opens the full-size chart, free to save or print.
One-page guide: Common Reasons Asthma Claims Are Denied
Four common asthma denial categories involving diagnosis, nexus, medication classification, and severity documentation. Opens the full-size chart, free to save or print.
Why These Claims Get Denied
Beyond the general "no nexus" and "no diagnosis" reasons, a few specific denial patterns in the published decisions are worth calling out on their own.
- Conceded toxic exposure, but no medical link. Even where the VA does not dispute that a veteran had toxic or burn-pit exposure, a claim can still be denied when the medical opinion in the file finds no connection, for example when the asthma is characterized as allergy-induced with an onset well after the exposure. Conceded exposure is not the same as an automatic win outside the presumptions.
- A diagnosis that turns out to be something else. A veteran who believed he had asthma, but whose actual diagnosis was chronic obstructive pulmonary disease, cannot rely on an asthma presumption or an asthma rating; the current-diagnosis requirement applies to the specific condition claimed, not a related one.
- The veteran's own belief about the cause, without a doctor's opinion behind it. Outside the presumptions, VA treats the cause of asthma as a medical question. A personal opinion that service or exposure caused the condition, without a supporting nexus opinion, does not carry a direct claim on its own.
- Assuming August 5, 2021 caps every particulate-matter asthma claim. It caps grants that REST ON 38 CFR 3.320, because 38 CFR 3.114(a) will not reach behind a liberalizing rule's own effective date. It does not cap a grant on a direct basis, where 38 CFR 3.400 governs and the date can be far earlier. If your records show asthma in service or continuous symptoms since, the direct theory is worth pleading alongside the presumption precisely because of the date.
- Rating or effective-date fights without the facts to support them. When there was no pending claim on file during the gap in question, an earlier effective date has been denied on that basis alone. And near-normal breathing tests paired with only intermittent inhaler use have kept ratings at 10 percent; the Board will not go higher without qualifying FEV-1 or FEV-1/FVC results, daily medication, or documented steroid courses in the record.
- A severance notice that goes unanswered. Once VA severs service connection for asthma, the veteran generally cannot later obtain an earlier effective date or an added benefit tied to that service connection. A proposed severance is serious and should be addressed head on, not ignored, ideally with the help of an accredited representative.
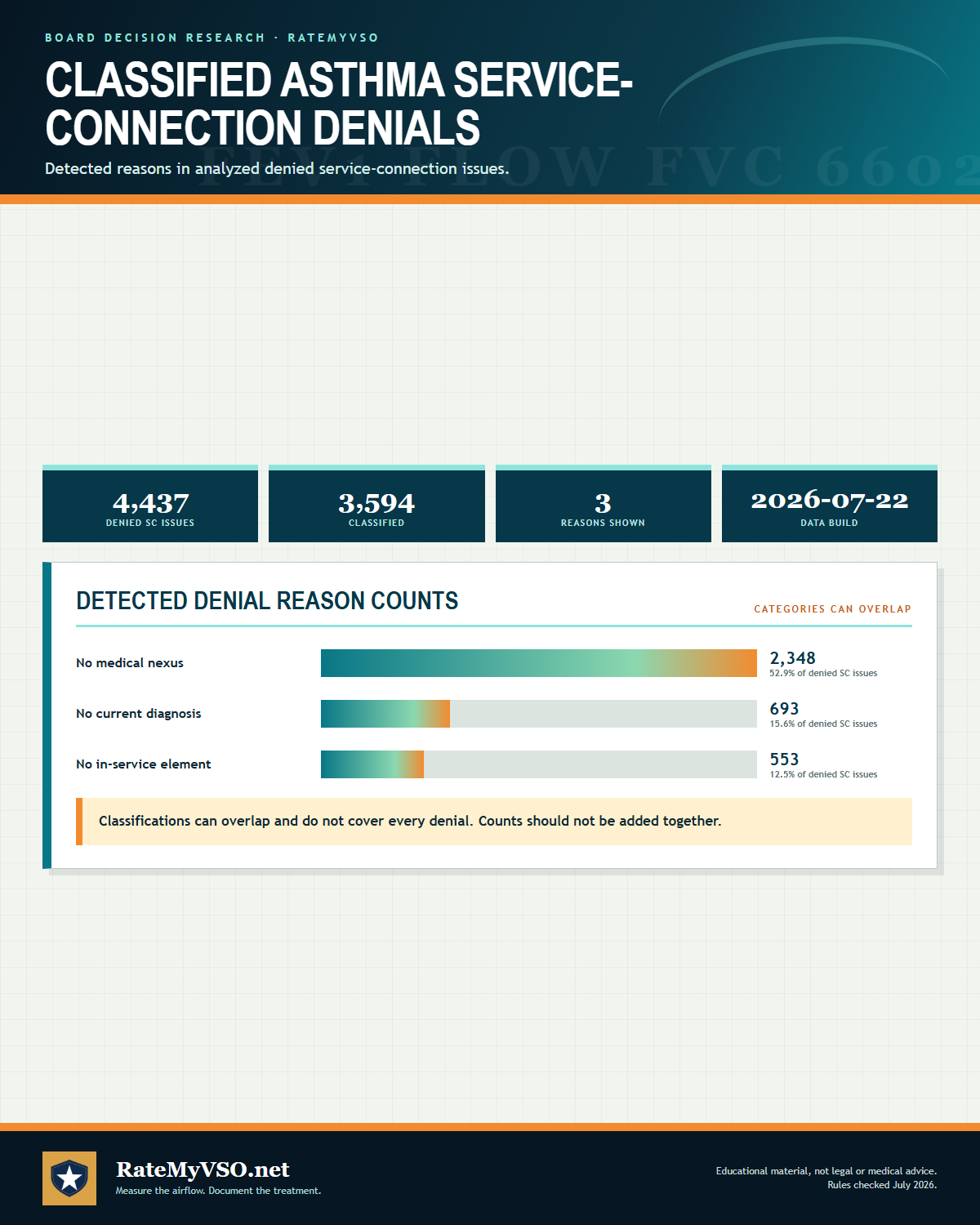 One-page guide: Classified Asthma Service-Connection Denials
Overlapping nexus, diagnosis and in-service-element classifications across 4,033 of 4,456 denied asthma service-connection issues. Opens the full-size chart, free to save or print.
One-page guide: Classified Asthma Service-Connection Denials
Overlapping nexus, diagnosis and in-service-element classifications across 4,033 of 4,456 denied asthma service-connection issues. Opens the full-size chart, free to save or print.
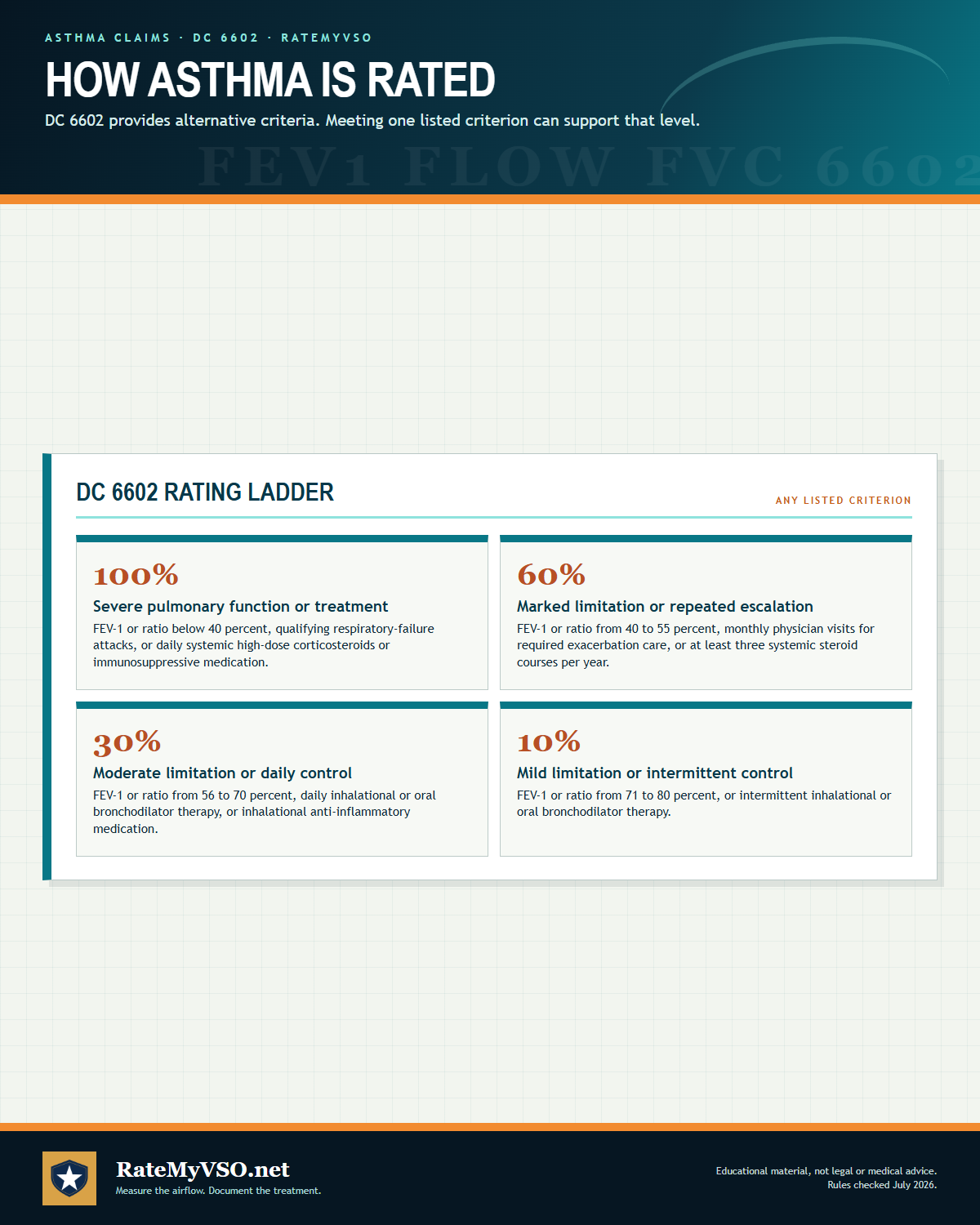
DC 6602 Rating Levels: Bronchial Asthma
The full schedule entry is "6602 Asthma, bronchial" under 38 CFR 4.97. The ladder runs 10, 30, 60, and 100 percent. The criteria below are reproduced verbatim from the current regulation. Remember that each level is satisfied by meeting any one of its listed criteria.
Go deeper: open the full bronchial asthma breakdown- What the VA measures at your C&P exam
- Evidence that has won at the Board
- Inside the rater's playbook: grant, denial, and remand rates
- Secondary condition map
Because each level can be reached by a single qualifying criterion, the medication and treatment-frequency paths are worth checking against your records every time. A veteran whose FEV-1 sits in the 30 percent range on paper can still meet the 60 percent level if a physician treats monthly exacerbations or prescribes three or more courses of systemic steroids a year. Intermittent inhaler use with near-normal breathing tests, on the other hand, tends to hold a rating at 10 percent; going higher takes qualifying FEV-1 or FEV-1/FVC results, daily medication, or documented steroid courses.
| Rate | Breathing-number path (any one) | Treatment path (any one) |
|---|---|---|
| 100% | FEV-1 under 40% predicted, or FEV-1/FVC under 40% | Daily high-dose systemic steroids or immunosuppressives, or more than weekly attacks with respiratory failure |
| 60% | FEV-1 40 to 55% predicted, or FEV-1/FVC 40 to 55% | At least monthly physician visits for exacerbations, or 3 or more systemic steroid courses per year |
| 30% | FEV-1 56 to 70% predicted, or FEV-1/FVC 56 to 70% | Daily inhalational or oral bronchodilator, or inhalational anti-inflammatory |
| 10% | FEV-1 71 to 80% predicted, or FEV-1/FVC 71 to 80% | Intermittent inhalational or oral bronchodilator |
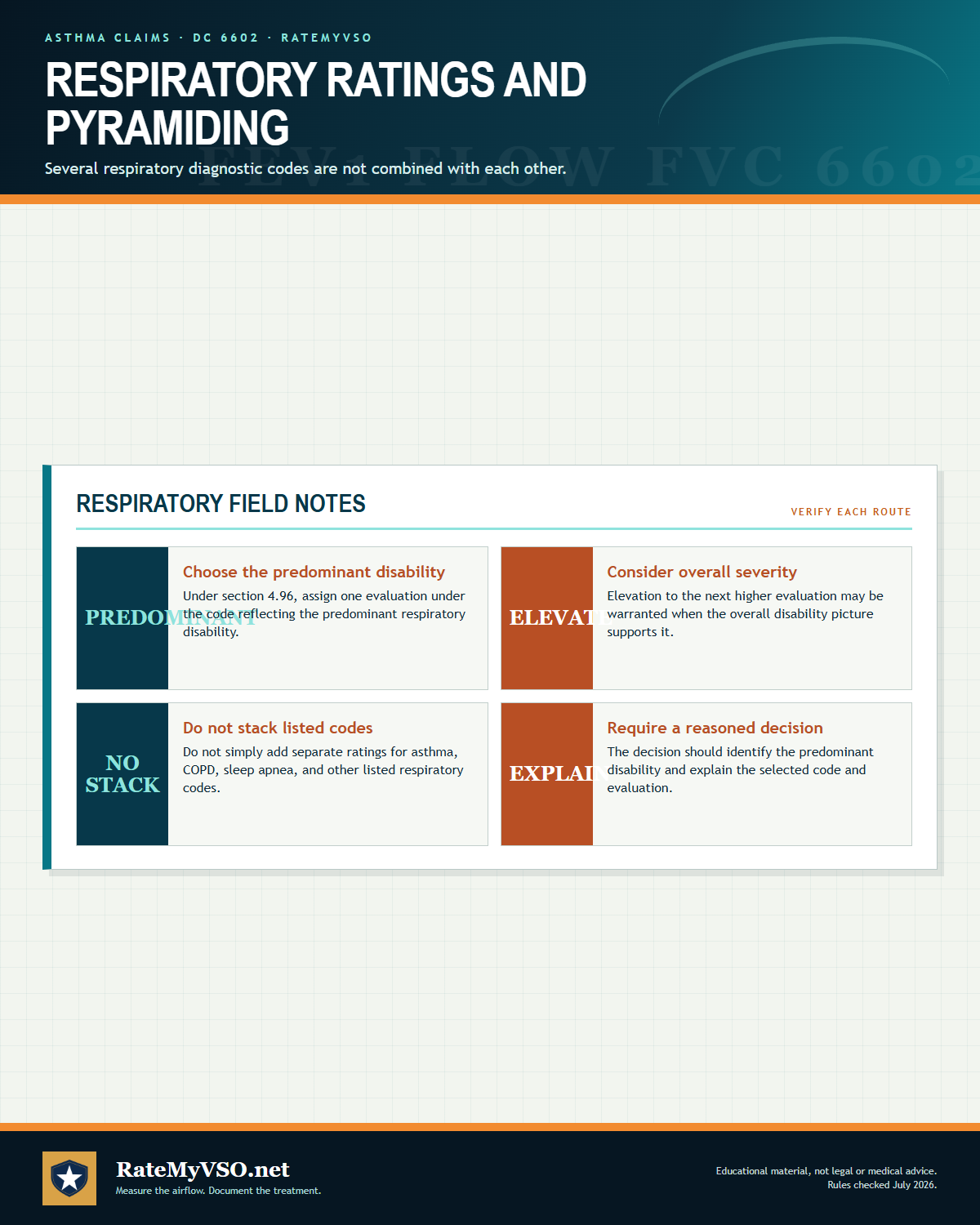 One-page guide: Respiratory Ratings and Pyramiding
Explanation of predominant respiratory disability, elevation, prohibited stacking, and decision reasoning. Opens the full-size chart, free to save or print.
One-page guide: Respiratory Ratings and Pyramiding
Explanation of predominant respiratory disability, elevation, prohibited stacking, and decision reasoning. Opens the full-size chart, free to save or print.
Pyramiding and Rating Separately
The VA's pyramiding rule at 38 CFR 4.14 bars paying twice for the same symptoms. For respiratory conditions, 38 CFR 4.96(a) adds a specific limit: ratings under several respiratory diagnostic codes (the list includes DC 6600 through 6817 and 6822 through 6847, among them asthma at 6602) generally cannot be combined with each other. Instead, when more than one of those conditions is present, a single rating is assigned under the diagnostic code that reflects the predominant disability, with elevation to the next higher evaluation where the severity of the overall disability warrants it. That elevation clause is part of the rule and is easy to overlook: being held to one code does not mean being held to what that one code would pay in isolation.
In practice this means asthma and a second obstructive lung condition such as chronic bronchitis or emphysema are usually evaluated together under the one code that best captures the overall breathing impairment, rather than stacked as separate percentages. Conditions outside the respiratory schedule, such as a separately diagnosed sleep apnea, GERD, or a mental-health condition, are rated under their own diagnostic codes and combined under 38 CFR 4.25, as long as the same symptoms are not counted twice.
Common Mistakes
Patterns the published decisions and the regulation flag:
- Submitting only pre-bronchodilator PFT numbers, or a breathing test with no bronchodilator step at all. 38 CFR 4.96(d) generally requires post-bronchodilator values for rating, and missing or mislabeled values can lock in a lower percentage.
- Not realizing the rating can be driven by medication alone. Daily bronchodilator or inhaled anti-inflammatory use supports 30 percent, intermittent systemic steroid courses (three or more per year) support 60 percent, and daily high-dose systemic steroids or immunosuppressives support 100 percent, independent of the FEV-1 number.
- Confusing inhaled corticosteroids with systemic corticosteroids. An inhaled corticosteroid is an inhalational anti-inflammatory (30 percent tier). Oral or injected steroids are systemic (60 to 100 percent tiers). This systemic-versus-inhalational wording is the most outcome-determinative line in the schedule.
- Filing a direct claim with no nexus evidence. Lack of a nexus is the leading denial reason for asthma, and appeals were granted at a markedly higher rate with a private nexus opinion in the file.
- No documented asthma at the exam and no verified history of attacks. The 6602 Note expressly requires a verified history of asthmatic attacks in the record when current findings are absent.
- Assuming a 10-year diagnosis deadline still blocks a PACT Act claim. That window came from the superseded 2021 particulate-matter rule. The current VA.gov burn pit presumptive standard is "diagnosed after service" for qualifying airborne-hazard service.
- Overlooking secondary pathways in both directions. Asthma claimed secondary to service-connected rhinitis or sinusitis, and obstructive sleep apnea claimed secondary to service-connected asthma, are both well-represented in the data.
- Missing or rescheduling a VA examination without good cause. When the exam needed to decide the claim is not attended and there is no good cause, the claim can be denied as a matter of law under 38 CFR 3.655. If you truly cannot attend, tell VA why and ask to reschedule before the appointment, not after.
Do's and Don'ts
A condensed version of everything above, in the order it actually matters when you sit down to build your file.
- Check whether you served in the Southwest Asia theater, the Gulf War era, or another covered location for a burn pit or particulate-matter presumption, often the fastest path to a grant.
- Get or confirm a current asthma diagnosis in writing from a VA or private doctor, in the exact terms of the condition you're claiming.
- Describe when your breathing problems started and that they have continued since service, in your own words.
- Ask fellow service members or family for statements about your symptoms during and after service.
- Point out when a VA opinion relies only on silent service records or a lack of old records, that basis alone does not defeat credible lay evidence of continuous symptoms.
- Attend every scheduled VA examination; if you truly cannot, ask to reschedule and explain your good cause before the appointment.
- Collect your pulmonary function tests and a full list of your asthma medications and doses, especially if you want a higher rating.
- Get a private nexus opinion, or a pulmonologist's letter, when the presumptions don't apply and you need to prove the medical link yourself.
- Address a severance notice head on and promptly, ideally with an accredited representative.
- If you were denied before, file a Supplemental Claim with new and relevant evidence rather than starting over.
- Don't assume conceded toxic exposure alone proves your asthma, outside the presumptions you still need a medical opinion that finds an actual link.
- Don't rely on a past label if your actual current diagnosis is a different respiratory condition, such as COPD, a presumption still requires the current diagnosis to match.
- Don't assume August 5, 2021 is the earliest date available. It binds a grant made under 38 CFR 3.320; a direct-service-connection grant is governed by 38 CFR 3.400 instead and can be earlier.
- Don't skip or reschedule your VA exam without telling VA why, a missed exam can end the claim as a matter of law.
- Don't count on a rating increase without qualifying breathing numbers, daily medication, or steroid courses to back it up.
- Don't ignore a notice that VA is proposing to sever your service connection, it forecloses later effective-date and benefit arguments if left unanswered.
- Don't confuse an inhaled corticosteroid with a systemic one when describing your medications, the wording changes the tier.
- Don't file with only pre-bronchodilator PFT numbers if a post-bronchodilator test is available.
 One-page guide: Two Independent Rating Paths
Comparison of pulmonary-function, treatment, and attack-based routes under DC 6602. Opens the full-size chart, free to save or print.
One-page guide: Two Independent Rating Paths
Comparison of pulmonary-function, treatment, and attack-based routes under DC 6602. Opens the full-size chart, free to save or print.
How the Rating Mechanics Work
DC 6602 is unusual because each rating level lists several independent ways to qualify, joined by the word "or." You do not have to meet every criterion in a level. Meeting any single one of them is enough to reach that percentage. The VA assigns the highest level your evidence supports.
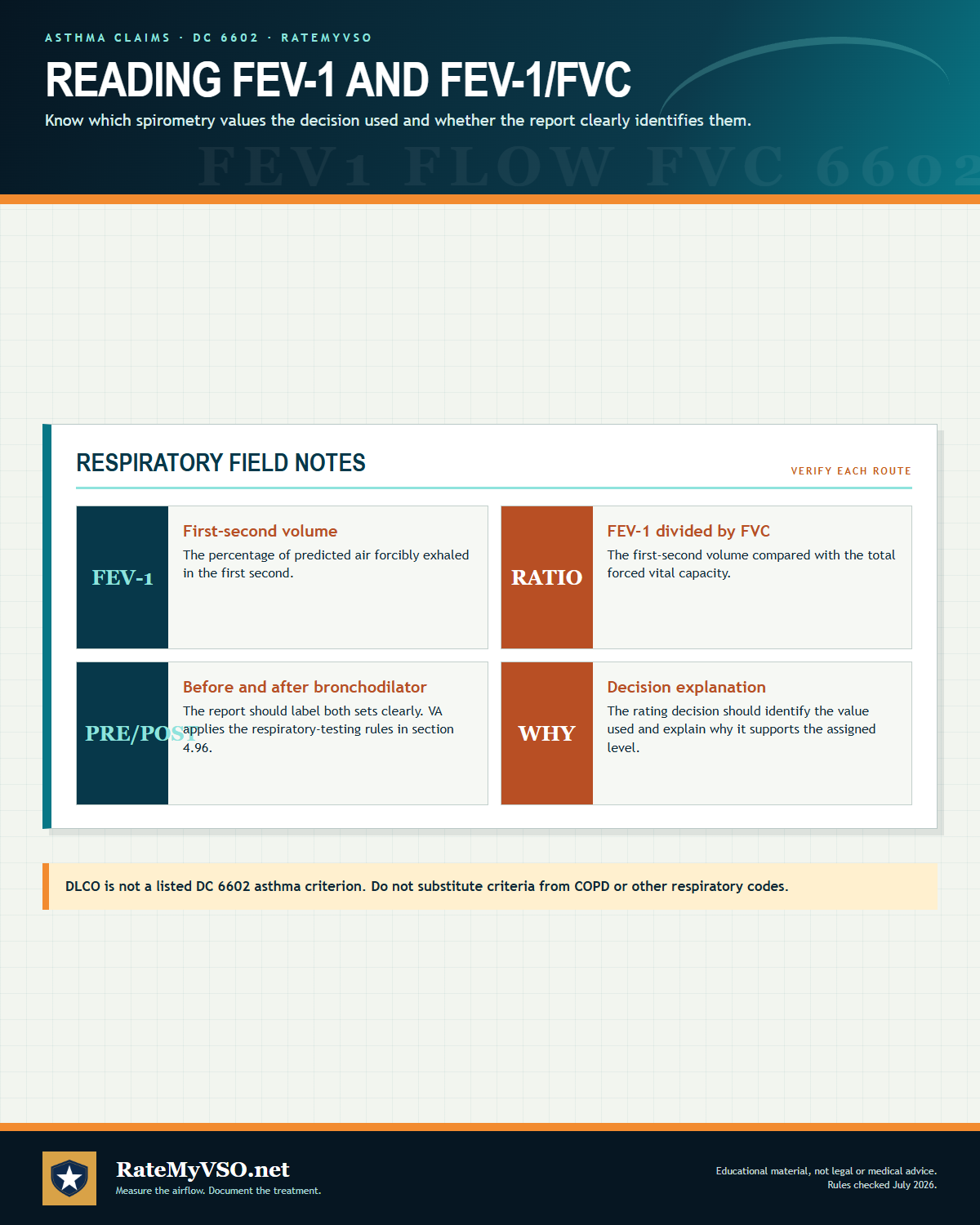
The dual pulmonary-function thresholds
Two breathing numbers can each independently set the rating: the FEV-1 (percent predicted) and the FEV-1/FVC ratio (a percentage). The thresholds run in parallel. For example, an FEV-1 of 56 to 70 percent predicted supports 30 percent, and so does an FEV-1/FVC ratio of 56 to 70 percent, separately. Because the two can disagree, the rule below for which test the rater uses matters.
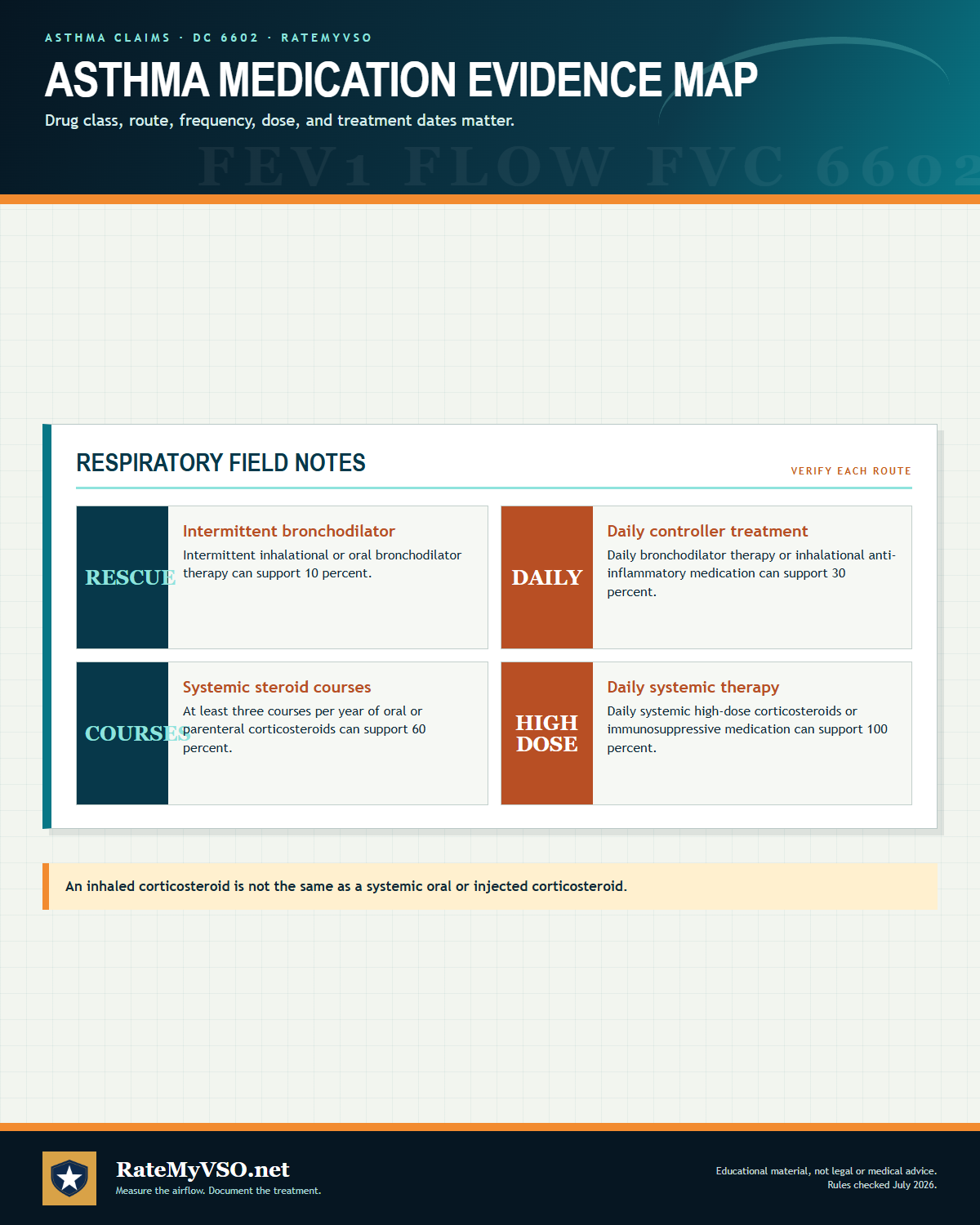
The parallel medication criteria (often the higher path)
Alongside the breathing numbers, the type of treatment you require can drive the rating on its own, and frequently lands higher than the numbers suggest. The schedule reads:
- 30 percent: daily inhalational or oral bronchodilator therapy, or inhalational anti-inflammatory medication (this includes daily inhaled corticosteroids).
- 60 percent: at least monthly visits to a physician for required care of exacerbations, or intermittent (at least three per year) courses of systemic (oral or parenteral) corticosteroids.
- 100 percent: daily use of systemic (oral or parenteral) high-dose corticosteroids or immunosuppressive medications, or more than one attack per week with episodes of respiratory failure.
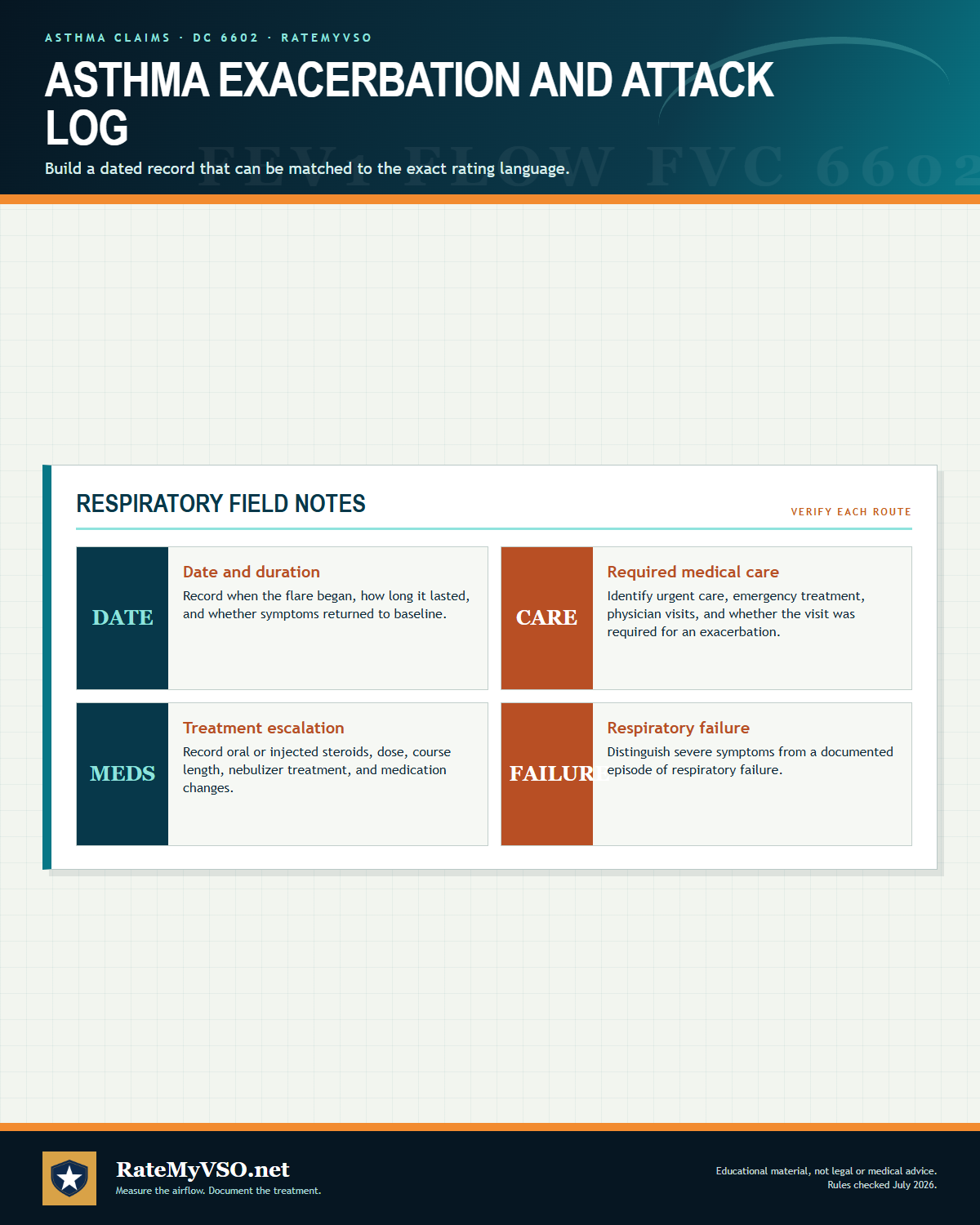 One-page guide: Asthma Exacerbation and Attack Log
Four-part log for attack dates, required medical care, treatment escalation, and documented respiratory failure. Opens the full-size chart, free to save or print.
One-page guide: Asthma Exacerbation and Attack Log
Four-part log for attack dates, required medical care, treatment escalation, and documented respiratory failure. Opens the full-size chart, free to save or print.
The post-bronchodilator PFT rule
Post-bronchodilator studies are generally required when pulmonary function tests are done for rating purposes (an exception applies when pre-bronchodilator results are normal, or when the examiner explains why a post-bronchodilator test should not be done). (see 38 CFR 4.96(d)) When evaluating based on PFTs, the rater uses the post-bronchodilator results, unless those results were poorer than the pre-bronchodilator results, in which case the pre-bronchodilator values are used. If different tests disagree and would yield different ratings, the examiner identifies the result that most accurately reflects the level of disability.
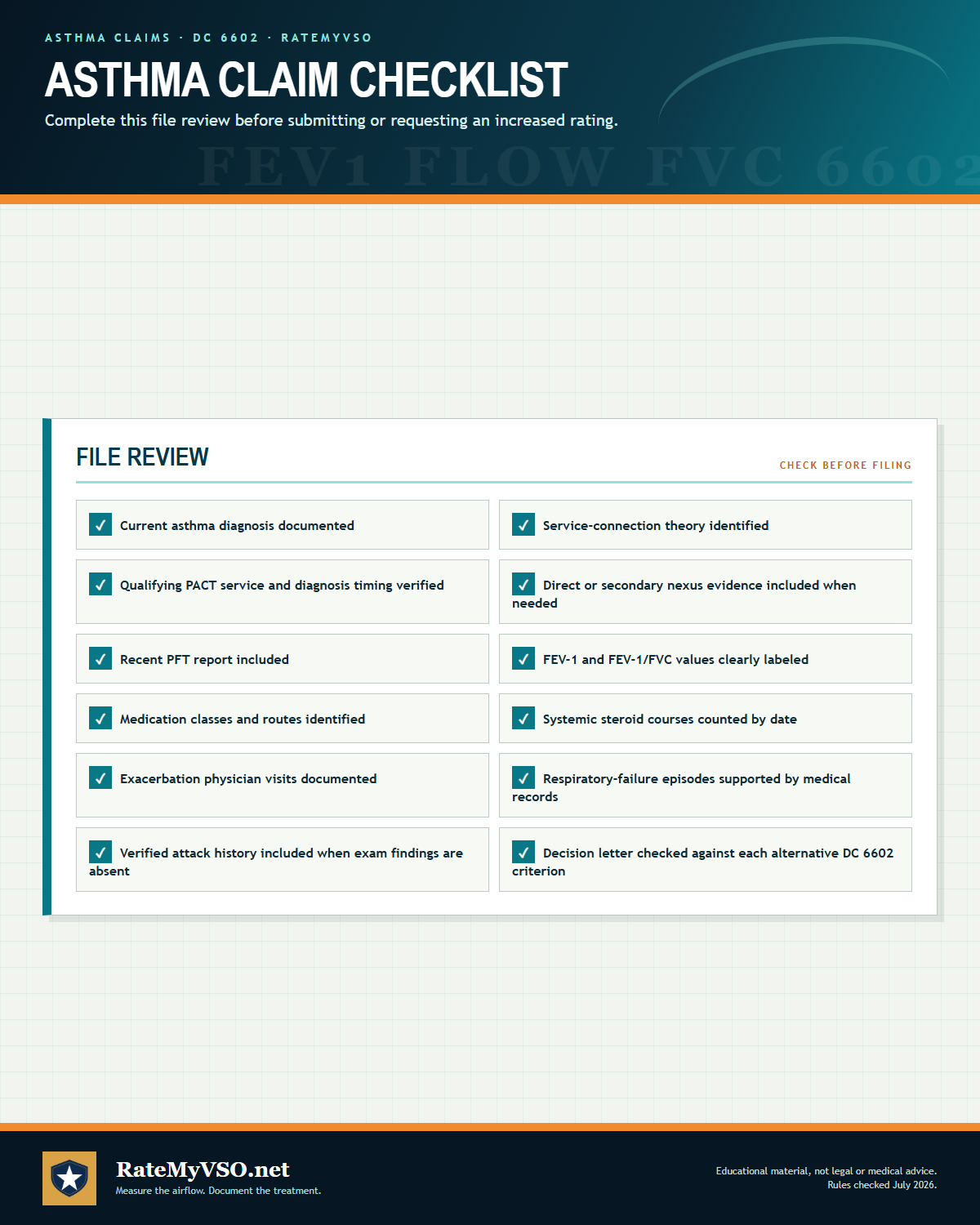 One-page guide: Asthma Claim Checklist
Twelve-item asthma claim checklist covering diagnosis, service connection, PFT, medications, attacks, and decision review. Opens the full-size chart, free to save or print.
One-page guide: Asthma Claim Checklist
Twelve-item asthma claim checklist covering diagnosis, service connection, PFT, medications, attacks, and decision review. Opens the full-size chart, free to save or print.
Quick Checklist Before You File
Bring these together before you submit anything.
- Get or confirm a current asthma diagnosis in writing from a VA or private doctor.
- Check whether you served in the Persian Gulf, Southwest Asia, or another covered location for a burn pit or particulate-matter presumption.
- Write down when your breathing problems started and that they have continued since service.
- Ask fellow service members or family for statements about your symptoms during and after service.
- Attend every scheduled VA examination; if you truly cannot, ask to reschedule and explain your good cause.
- Collect your pulmonary function tests (with clearly labeled pre- and post-bronchodilator values) and a full list of your asthma medications and doses if you want a higher rating.
- A nexus opinion or pulmonologist's letter, if you are not relying on a presumption, that explains the connection to service or to a service-connected condition.
- If you disagree with a decision, file a Supplemental Claim (VA Form 20-0995) with new and relevant evidence.
For the mechanics of actually submitting the claim, see the Standard Claim Guide and the Fully Developed Claim Guide (filing with all your evidence up front can speed up the decision).
The Claims Process, Step by Step
Once you file, your claim moves through a series of hand-offs. Understanding who does what helps you know who to contact, and what to expect, at each stage.
- You file the claim. Directly with VA, through VA.gov, or with the help of an accredited representative.
- VA acknowledges the claim and assigns it for development. A Veteran Service Representative (VSR) is assigned to gather your service treatment records, VA and private medical records, and any other evidence needed.
- The VSR orders a Compensation & Pension (C&P) exam if one is needed. Not every claim requires one, especially a straightforward PACT Act or 38 CFR 3.320 presumptive claim with a clear current diagnosis, but most direct and secondary asthma claims do.
- The C&P exam is conducted. By a VA clinician or a contracted examiner, who completes a Disability Benefits Questionnaire (DBQ) documenting the diagnosis, pulmonary function results, medication regimen, and, where relevant, a nexus opinion.
- The file goes to a Rating Veteran Service Representative (RVSR), the "rater." The rater reviews the complete file, including the exam results, and decides whether service connection is warranted and at what percentage.
- A senior reviewer may review the decision before it's finalized, depending on the complexity of the claim.
- VA issues the decision letter. This states whether the claim is granted or denied, the rating percentage if granted, and the reasons behind the decision.
- If you disagree, you choose an appeal lane. Higher-Level Review, Supplemental Claim, or a Board appeal, covered later in this guide.
Who's who: VSO vs. VSR vs. Rater vs. C&P Examiner
Your VSO
An accredited representative from a veterans service organization, or an accredited attorney or claims agent. Not a VA employee. Helps you prepare, gather evidence, and file, and can represent you through an appeal. Has no authority to decide your claim.
VSR (Veteran Service Representative)
VA staff who "develops" your claim: requests records, schedules the C&P exam, and assembles the file. Does not decide the rating.
Rater (RVSR)
VA staff who reviews the completed file and makes the actual decision, service connection or denial, and the percentage. This is the person whose judgment the decision letter reflects.
C&P Examiner
A VA clinician or a contracted medical examiner who conducts the exam and completes the DBQ. Documents findings and, where asked, a nexus opinion. Does not decide the claim.
For the full walkthrough of every stage with more detail, see Inside Your Claim and Claim Stages.
 One-page guide: Asthma C&P Examination Guide
Asthma C&P examination preparation covering medications, steroid courses, exacerbation visits, and attack history. Opens the full-size chart, free to save or print.
One-page guide: Asthma C&P Examination Guide
Asthma C&P examination preparation covering medications, steroid courses, exacerbation visits, and attack history. Opens the full-size chart, free to save or print.
Diagnostic Tests and Your C&P Exam
Because DC 6602 keys on both objective numbers and treatment, the exam and the supporting records center on a short list of items:
- Spirometry / pulmonary function tests: these report FEV-1 (percent predicted) and the FEV-1/FVC ratio, the primary objective criteria in the rating table.
- Post-bronchodilator results: per 38 CFR 4.96(d)(4) and (d)(5), post-bronchodilator values are used for rating unless they were poorer than the pre-bronchodilator values, in which case the pre-bronchodilator values are used.
- The VA Respiratory Conditions DBQ: the examiner records FEV-1/FVC, the treatment regimen, attack frequency, and exacerbations on the Disability Benefits Questionnaire. See the DBQ Guide for how these forms work, including whether a private DBQ completed by your own doctor can be submitted instead of relying solely on a VA exam.
- Documentation of the treatment regimen: because medication type independently drives the rating, the records should distinguish inhalational bronchodilator therapy (10 to 30 percent), inhalational anti-inflammatory (30 percent), intermittent systemic corticosteroid courses of three or more per year (60 percent), and daily high-dose systemic corticosteroids or immunosuppressives (100 percent).
- Records of physician visits and exacerbations: at least monthly visits for required care of exacerbations supports 60 percent, and episodes of respiratory failure support 100 percent.
- A verified history of asthmatic attacks: required by the 6602 Note when no asthma findings are present at the time of exam.
- Methacholine or bronchoprovocation challenge testing and chest imaging: these can appear when the diagnosis itself is contested, though they are not rating-table criteria. The VA's evaluation of respiratory conditions, including the testing and the systemic-versus-inhalational distinction, is governed by M21-1, Part V, Subpart iii, Chapter 4, Section A (Respiratory Conditions).
Before your C&P exam, bring a clear, specific account of your symptoms and be consistent with what's already in your medical records and prior statements. For a full walkthrough of what to expect and how to prepare, see the C&P Exam Prep Guide.
Reading Your Decision Letter, and What to Do If Denied
Your decision letter has two parts: a narrative section explaining the reasoning (often called "reasons and bases"), and a codesheet showing the actual rating percentage, the effective date, and the diagnostic code used. See the Reading Your Decision Letter Guide for how to find and interpret each part, or use the Letter Interpreter tool to upload your own letter and get a plain-English breakdown.
If your claim is denied, the rating is lower than you expected, or VA proposes to sever a service connection you already have, you have three main lanes:
- Supplemental Claim: refile with new and relevant evidence, such as a new nexus opinion, an updated pulmonary function test, or a pulmonologist's letter. See Supplemental Claim Guide.
- Higher-Level Review (HLR): a senior reviewer looks at the same evidence again for a difference of opinion, no new evidence is added. See HLR Guide.
- Board Appeal: your case goes to a Veterans Law Judge at the Board of Veterans' Appeals, with options for a direct review, an evidence docket, or a hearing. See Board Appeal Guide.
Not sure which lane fits your situation? See the Appeals decision guide for a side-by-side comparison of all three.
 One-page guide: Increased Rating and Effective-Date Review
Increased-rating and effective-date review based on worsening criteria, dated evidence, governing authority, and reduction procedure. Opens the full-size chart, free to save or print.
One-page guide: Increased Rating and Effective-Date Review
Increased-rating and effective-date review based on worsening criteria, dated evidence, governing authority, and reduction procedure. Opens the full-size chart, free to save or print.
After You Win: Maintaining Your Rating and Getting the Effective Date Right
Many asthma appeals are not about getting service connection at all, they are about the rating percentage or the effective date once you're already service connected. Your rating is decided mostly by the breathing-test numbers and by your medications, so keeping consistent, well-documented treatment, ongoing pulmonary function testing, and a current medication list, protects both your current rating and any future request for an increase. When asthma is granted under the 38 CFR 3.320 particulate-matter rule specifically, the effective date will not reach behind that rule's own August 5, 2021 start, because 38 CFR 3.114(a) does not allow it; a grant on a direct basis is not limited that way. Effective-date fights are otherwise limited by the facts on file; if there was a gap with no pending claim, an earlier date is unlikely to be granted for that period.
A grant is not always the end of the story on the VA's side either. Not every rating gets reexamined, and VA can also propose to sever a service connection it previously granted, which is a serious action that should be addressed immediately rather than ignored. Understand when a rating becomes protected from future review (including Permanent and Total status) and what to do if VA proposes to reduce or sever it. See Protect Your Rating and Future Reexaminations for the specifics.
If your asthma worsens after the initial grant, for example needing daily systemic steroids where you once needed only an inhaler, you can file for an increased rating with your updated pulmonary function tests and medication records. See the Rating Increase Guide.
Common Secondary Conditions
Asthma sits in the middle of a web of related conditions. It can be the downstream condition another service-connected disability caused, and it can be the upstream cause that supports a further claim. All of the rates below are grant rates from published BVA decisions, paired with the number of appeals.
Conditions that can cause or contribute to asthma (asthma as the secondary)
Claims where asthma was argued as secondary to an already service-connected condition, such as rhinitis, sinusitis, or GERD above. This is the "ways to connect via another condition" list:
Conditions asthma can cause or contribute to (asthma as the primary)
We found each bar is the published BVA grant rate for a condition claimed secondary to asthma, with the number of decisions below it:
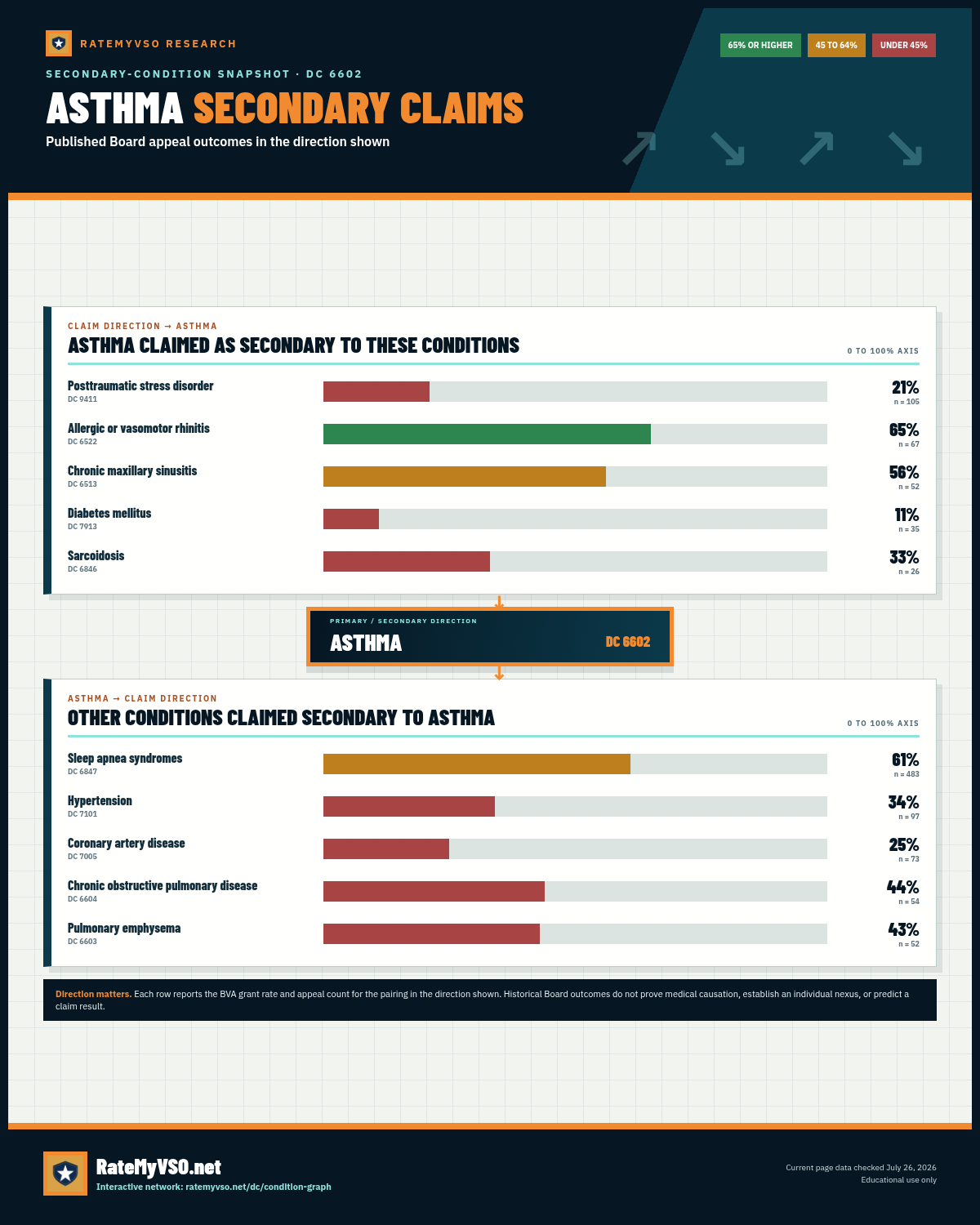 One-page guide: Asthma Secondary-Claim Snapshot
Two-direction secondary-claim snapshot for ASTHMA, showing BVA grant rates and appeal counts for conditions claimed toward and away from ASTHMA. Opens the full-size chart, free to save or print.
One-page guide: Asthma Secondary-Claim Snapshot
Two-direction secondary-claim snapshot for ASTHMA, showing BVA grant rates and appeal counts for conditions claimed toward and away from ASTHMA. Opens the full-size chart, free to save or print.
Quick Reference Tables
Presumptive and Secondary Connection Pathways
| Pathway | Mechanism | Evidence Needed |
|---|---|---|
| PACT Act burn pit presumptive | Qualifying airborne-hazard or burn pit exposure; asthma diagnosed after service | Proof of qualifying service + current asthma diagnosis (no nexus opinion needed) |
| 38 CFR 3.320 particulate-matter presumptive | Presumed exposure to fine particulate matter, Gulf War theater | Proof of qualifying service + current asthma diagnosis. A grant resting on this rule takes an effective date no earlier than Aug. 5, 2021 (38 CFR 3.114(a)); a direct grant is not bound by that |
| Rhinitis/sinusitis (DC 6522, 6510) | "United airway" theory: upper-airway inflammation reduces lower-airway function | Nexus opinion linking the service-connected upper-airway condition to the asthma |
| GERD (DC 7206) | Refluxed acid irritates the airway and worsens asthma symptoms | Nexus opinion addressing the GERD-asthma link, either direction |
From Filing to Decision: Who Does What
| Role | Does | Decides your rating? |
|---|---|---|
| VSO / accredited representative | Helps prepare, gather evidence, and file; represents you on appeal | No |
| VSR | Develops the claim: orders records and the C&P exam | No |
| C&P Examiner | Conducts the exam, completes the DBQ, may give a nexus opinion | No / but has a strong impact |
| Rater (RVSR) | Reviews the full file and decides service connection and percentage | Yes |
Frequently Asked Questions
Is asthma a PACT Act burn pit presumptive condition?
Does my asthma have to have started within 10 years of service?
My breathing test numbers look fine, but I take a daily inhaler. Can I still be rated?
What is the difference between inhaled and systemic steroids for the rating?
Why does the VA want a post-bronchodilator breathing test?
What is the strongest way to connect asthma to another service-connected condition?
What happens if I miss my C&P exam?
What if VA is trying to take away my asthma service connection?
Related Tools and Guides
Sources
- 38 CFR 4.97, Diagnostic Codes 6600 and 6602, rating bronchitis and bronchial asthma
- 38 CFR 4.96, special provisions for evaluating respiratory conditions (post-bronchodilator PFT rule, pyramiding limit)
- 38 CFR 3.303, basic rules for service connection
- 38 CFR 3.310, secondary service connection
- 38 CFR 3.320, presumptive service connection for asthma from fine particulate matter, effective August 5, 2021
- 38 CFR 3.380, diseases of allergic etiology, including bronchial asthma
- 38 CFR 3.317, Persian Gulf War undiagnosed illness and medically unexplained chronic multi-symptom illness
- 38 CFR 3.307 and 3.309, chronic disease presumptions and continuity of symptoms
- 38 CFR 3.102 and 38 USC 5107(b), benefit of the doubt
- 38 CFR 3.104(c), VA favorable findings bind the Board
- 38 CFR 3.655, effect of failing to report for a VA examination
- 38 CFR 3.400 and 3.114, effective dates, including liberalizing laws
- PACT Act, Pub. L. 117-168, presumptions for burn pit and toxic exposure
- Buchanan v. Nicholson, 451 F.3d 1331 (Fed. Cir. 2006), VA cannot rely solely on the absence of records to reject credible lay evidence of continuous symptoms
- VA.gov, the PACT Act and your VA benefits (burn pit and airborne-hazards presumptive conditions)
- VA.gov, burn pit and other airborne hazards exposures
- M21-1, Part V, Subpart iii, Chapter 4, Section A (Respiratory Conditions)